
Teenage hormone push
Australia's gender-affirming treatment guideline was altered to mainstream the supply of cross-sex hormones while protecting doctors from litigation


A contentious change to Australian treatment guidelines was “carefully crafted” to discourage medical insurers from denying cover to general practitioners in primary care (GPs) who are willing to start minors on cross-sex hormones with no specialist backup, according to an insider’s account.
The November 2023 change encouraging GP-driven hormones calls into question the “multidisciplinary team” rhetoric of the 2018 “Australian standards of care” treatment guidelines for minors issued by the Royal Children’s Hospital (RCH) Melbourne.
This multidisciplinary rhetoric has been relied upon by Australian health authorities and the local gender medicine lobby to dismiss the need for reforms Down Under following England’s historic Cass review of gender dysphoria care.
The change to the Australian guidelines was made without any public explanation by the RCH Melbourne gender clinic or any citation of studies favouring irreversible hormones for teenagers via primary care.1
The rationale for the change is not given in the guideline itself. The fact of the change is signalled by a new paragraph under “Acknowledgements,” noting those involved in “the updated GP section in Version 1.4.”
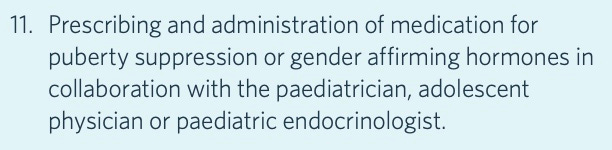
Screenshot: “Roles of the GP” excerpt, from the RCH Melbourne treatment guideline before November 2023
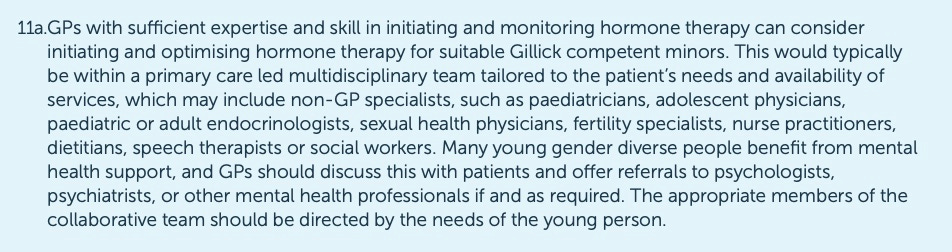
Screenshot: “Roles of the GP” excerpt, from the RCH Melbourne treatment guideline since November 2023
Optimal care
The “gender-affirming” RCH guideline, which is used across Australia, still stipulates “a co-ordinated, multidisciplinary team approach” as “the optimal model of care.” The guideline has been endorsed by the Australian Professional Association for Trans Health (AusPATH).
AusPATH’s international counterpart, the World Professional Association for Transgender Health (WPATH), stands accused of seeking to suppress reviews confirming the low quality of the evidence base for gender medicine, while allowing its latest treatment guideline, known as SOC-8, to be influenced by political pressure, litigation tactics, considerations of insurance coverage and the shielding of clinicians from legal liability.
Unguarded emails and group discussions within WPATH have become public as a result of forensic manoeuvres in a US Supreme Court test case over a state ban on medicalised gender change for minors; the judges are to hear arguments in December.
“Malpractice insurance prices [in the US] are stopping small clinics from offering gender-affirming care to minors.”—News report, Time magazine, 21 December 2023
“Nearly two dozen [US] detransitioners have filed medical-malpractice and fraud lawsuits against care providers who oversaw their gender-transition treatment when they were minors or young adults… Insurance experts told The Post that successful detransitioner litigation might magnify this effect [of rises in medical insurance premiums] and threaten the financial viability of at least some smaller clinics.”—News report, The New York Post, 19 October 2024
First mover
The Australian guideline change followed a historic decision in May 2023 by medical insurer MDA National to deny cover to doctors in private practice who start minors on cross-sex hormones. The insurer said this risky intervention ought to be under the watch of “a multidisciplinary team in a hospital setting.” It also expressed scepticism about claims that detransition rates are low.
“We’re talking about people who are making life-changing decisions. So, our feeling is that that is a very high level of risk for an individual GP to take on their own,” MDA National’s president Dr Michael Gannon told newsGP last year.
Gender clinic teams in Australian state children’s hospitals have long waiting lists, and advocates for the gender-affirming treatment model are seeking to ramp up hormone supply to 16-17-year-olds and young adults through suburban GP practices and adolescent mental health organisations such as Orygen/Headspace.
The crucial new section in the current version 1.4 of the RCH Melbourne treatment guideline says—
“GPs with sufficient expertise and skill in initiating and monitoring hormone therapy can consider initiating and optimising hormone therapy for suitable Gillick-competent minors [also known as ‘mature minors’]. This would typically be within a primary care-led multidisciplinary team, which may include non-GP specialists such as paediatricians, adolescent physicians, paediatric or adult endocrinologists, sexual health physicians, fertility specialists… [Emphasis added.]”
In a GP group chat earlier this year about uncertain coverage by medical insurers, Sydney GP Portia Predny highlighted the “carefully crafted” wording of the guideline change.
The aim, she suggested, was to prevent medical insurers denying coverage with the “excuse” that the RCH guideline always, not just typically, requires a GP to have specialist backup. Dr Predny is among the members of an AusPATH working group2 whose contribution to the November 2023 change is acknowledged in the RCH guideline.
“We were specifically so careful in our wording of the updated guidelines to ensure that the recommendations around the involvement of a multidisciplinary team were open-ended enough to account for situations in which a mature minor might not need additional [specialist] involvement, as well as those circumstances in which specific services/specialists [such as endocrinologists] were not available,” she posted in the GP group chat.
She pointed out that the word “typically” was used in the November 2023 change to the roles of a GP, rather than “can only be,” and the term “may include” was chosen rather than “must include.”
The context for the group chat was continuing uncertainty about whether or not Avant, Australia’s largest medical insurer, would cover GPs initiating hormones for minors without specialist backup.
GPs following the gender-affirming treatment approach have cited conflicting messages from Avant representatives and complained of the short supply of specialists willing to take part in medical transition of minors.
This week, a spokesman for Avant told GCN there had been no change in the insurer’s position. However, he did not answer a direct question whether or not Avant would cover a GP who commences a minor on cross-sex hormones without specialist backup.
“[I]n the last year, several studies have shed light on the fact that gender dysphoria in adolescence is not a permanent diagnosis. At least three recent studies examined the diagnostic prevalence of the gender dysphoria diagnosis in youth. These studies found that as few as 40 per cent to 50 per cent of adolescents with a gender-related diagnosis retain that diagnosis after five to seven years, and trends indicate this number will continue to go down with longer follow-up…
“The finding of low diagnostic stability of the gender dysphoria diagnosis, and its poor predictive validity, greatly challenges the key premise that gender-dysphoric adolescents are ‘transgender’.”—Amicus brief for the US Supreme Court test case of US v Skrmetti, the Society for Evidence-based Gender Medicine, 3 September 2024
Video: Australian child and adolescent psychiatrist Dr Jillian Spencer discusses her concerns about the gender-affirming treatment model
Access medicine
News of the MDA National decision in May 2023 alarmed the gender medicine lobby group LGBTIQ Health Australia, whose access to federal Health Minister Mark Butler produced an “URGENT one-day turnaround” brief from his department on the issue, according to documents obtained under Freedom of Information law.
In a June 2023 article for the website AusDoc, Dr Predny reported that although MDA National’s policy shift did not amount to a “blanket ban” on gender medicalisation of minors, it “has still rattled GPs treating gender-diverse patients.”
In December last year, emeritus professor of law Patrick Parkinson wrote to Avant’s medico-legal team giving his opinion that it is unlawful for GPs to prescribe cross-sex hormones for minors without a formal diagnosis of gender dysphoria and the involvement of a multidisciplinary team.
“Treatment which could affect fertility in an otherwise healthy adolescent can only be authorised if it is for treatment of an illness or disease (following Re Marion),” Professor Parkinson wrote, citing a key High Court ruling.
“Gender dysphoria is understood to fall within this category, given its place still in [the diagnostic manual of psychiatry] DSM-5 as a disorder. A diagnosis of gender incongruence according to the [WHO diagnostic classification] ICD is not enough because that is not classified as a disorder.
“Furthermore, the [Australian Family Court] majority in Re Kelvin moved from their position that court approval was needed [before hormones were initiated] on the basis that the treatment would be provided by a multidisciplinary team in a hospital setting. GP treatment was not contemplated and it is difficult to imagine that the court would have approved it.”
In the 2017 re Kelvin case, which liberalised access to cross-sex hormones for minors, the judges relied on a draft version of the 2018 RCH treatment guideline.
“Revealed: over 200 transgender patients [in the UK] have been refused hormone care by GPs… While the reasons varied, the most common was that GPs ‘didn’t feel competent to prescribe it’.”—News report, QueerAF, 19 October 2024
“As GPs, we strive to deliver the highest standards of care as outlined in the [UK] General Medical Council’s Good Medical Practice. According to Paragraph 14 of this guidance, doctors are required to ‘recognize and work within the limits of their competence.’ In the case of transgender medicine, we feel that the complexities of hormone therapy and the associated monitoring required are beyond the scope of our expertise and capacity as a general practice.”—GP practice letter to a UK patient, shared anonymously on social media, October 2024
Cass Down Under
As AusPATH vice-president, Dr Predny was quoted in Australian media outlets discounting the local relevance of April’s final report from Dr Hilary Cass, the distinguished paediatrician whose 2020-24 review included an evaluation of international guidelines in which the RCH Melbourne guideline was judged not fit for use.
“In Australia, our guidelines for gender-affirming care for young people already prioritise holistic, individualised and person-centred care with the involvement of multidisciplinary teams of clinicians with all kinds of areas of expertise, to help and support young people to navigate their gender journey,” Dr Predny said in an Equality Australia media statement on the Cass review.
The statement, which included US activist talking points rebutted by Cass, did not mention the new GP-alone option for teenage hormones in the RCH guideline.
In April, ABC radio’s Health Report broadcast a program titled “Australia is not the UK” and suggesting that the relevance of Dr Cass’s report was confined to England, apart from her endorsement of a multidisciplinary approach, which listeners were told was already the Australian way.
Melbourne-based paediatric endocrinologist Dr Jacky Hewitt challenged these claims on Twitter.
Dr Hewitt, who gave evidence in a recent UK court case that a 15-year-old girl had been at risk of sudden death following a “dangerously high” dose of testosterone, said there were “primary care providers [such as GPs] prescribing cross-sex hormones to minors without any other specialist involvement.”
“So, the suggestion that hormone treatment is always only provided after careful multidisciplinary assessment is misinformed—both in Australia and elsewhere.”
She said the quality of assessment in gender clinics “varies greatly.”
The Cass report says: “Despite the agreement within the international guidelines on the need for a multidisciplinary team, and some commonalities between them in the areas explored during the assessment process, the most striking problem is the lack of any consensus on the purpose of the assessment process.”
Screenshot: Paediatric endocrinologist Dr Jacky Hewitt defends the relevance of the Cass report

Mainstreaming hormones
Anecdotal reports suggest that the trend of Australian GPs going it alone with hormones for teenagers is particularly pronounced in the state of Victoria.
In 2022, the number of new referrals to the RCH Melbourne gender clinic in Victoria fell by 23 per cent to 634. In the decade to 2021, referrals had risen 100-fold to 820.
Victoria’s former gay rights lobby, Thorne Harbour Health, has been running free-of-charge courses promising GPs “up-to-date knowledge about transgender and gender-diverse primary care.”
The course involves three two-hour sessions online and includes the prescribing of cross-sex hormones.
“As someone who has a prescription for testosterone and is in their 30s, I’m glad I went off social media, worked on my mental health, lost weight and decided I didn’t want to transition after all. If I didn’t know my own mind in my 30s, how can children?”—Forest Van Slyke, an author with autism, tweet, 21 October 2024
Branching out
Another factor in the decline of referrals to the RCH gender clinic, which takes patients up to age 16, may be a new “clinical pathway” to mental health group Orygen. This was funded by Victoria’s government in 2021.
The Orygen Transgender and Gender Diverse Service in Victoria is aimed at 12- to 25-year-olds and operates at five Headspace centres and via telehealth. It is promoted on the webpage of the RCH gender clinic.
According to the RCH clinic, this Orygen service “follows the WPATH guidelines and provides multidisciplinary support”.
The current WPATH guideline, SOC-8, abandoned minimum ages for gender medical interventions, including most surgery, following pressure from the US Biden Administration.
The guideline includes “eunuchs” as a gender identity and speaks of “their need for medically necessary gender-affirming care” in line with the “wish to eliminate masculine physical features, masculine genitals, or genital functioning.”
GCN sought comment from Dr Predny and RCH Melbourne. GCN does not dispute that gender-affirming clinicians believe their interventions benefit vulnerable young people.
A 2020 review of guidelines for primary care initiation of hormones with adults did not deliver an encouraging result. It noted that the “low quality” 2012 (SOC-7) guideline from the World Professional Association for Transgender Health was silent on whether cross-sex hormones could be initiated in primary care. The authors of the review said: “Historically, medical care for transgender people has been provided in highly specialized gender centers, where mental health professionals, endocrinologists or other specialists carried out appropriate assessment and subsequent treatment if necessary.” As for the RCH Melbourne guideline, the most recent studies on its reference list are from 2018. In May 2022, the then RCH gender clinic director Dr Michelle Telfer announced a project to undertake the first major revision of the guideline. In December that year Dr Telfer, who was lead author of the 2018 RCH guideline, stepped down as clinic director. In February 2023, the Australian Professional Association for Trans Health (AusPATH) said it would take charge of the guideline revision project. The status of that project is unknown. It is not clear whether RCH or AusPATH now bears ultimate responsibility for the guideline, although its four published authors were all from the RCH gender clinic and the hospital’s name and brand remains on the document.
The full name of the group is the AusPATH ASOCTG (Australian Standards of Care and Treatment Guidelines) GP Working Group.
I spent about a half a minute on the 'Headspace' website, a sample:
"Gender identity, like sexuality, is fluid, meaning it can change over time. This is completely normal. You don’t have to label your gender identity. However, if you choose to label your sexuality or gender it’s your choice; it’s what feels best for you; and when you’re ready - embrace and celebrate it!"
CREEPY NONSENSE!
Just to let you know, I wish I could claim compensation for the damage being done to my family, from our medical system, QLD health, and all the ideological lobby groups infiltrating all the support bodies for VERY vulnerable young people. Plus the support bodies themselves.
I have vulnerable children with diagnoses that need support from professionals and therapists, and who would benefit from some of the services delivered by NGO bodies like Headspace.
But because my children are so vulnerable I can't allow them anywhere near a whiff of any therapist, GP or paediatrician, having already seen them go backwards in their health and happiness due to the trans ideology being brought into the room. Which has confused one of my children's already confused state in dealing with significant trauma at the time. My children strongly defend the ideology, despite naturally developing out of it in everything except strong alliance to it.
I'm lucky. I'm a professional within the system. So I have been able to stay one step ahead of the ideology. But I've lost my job doing it, and my children's development both exceptionally delayed despite being brought and capable (one has very high iq but socially vulnerable). This is because I've been unable to access good professional care for them from someone like Jillian Spencer, or therapists who weren't able to tell me they were free of the ideology. And I've spent YEARS looking and trying them out.
So I can categorically sit here and say, on the strength of your article, that my intuition was correct in avoiding referral for my kids to places like headspace.
And
That from what you're saying, Headspace is a definite groomer of EXTREMELY vulnerable kids with terribly complex histories, ripe for the picking.
If they are kids like mine- unable to discern subtle feelings of 'something is off here', or hungry for acceptance and kindness, or looking for answers to their emotional discomforts.... they will be groomed as soon as they walk in the door.
This is terrifying.
I also think... how are we ever going to stop the tide, when these kids are the biggest fighters for the cause, and they are being recruited in droves?
Whether or not they have sensible, loving adults in their lives, who they respect.
They will listen to the authority figures, particularly when they are low enough to have to engage in attending places like Headspace, or therapist appointments- GO appointments, even.
Whether or not they have differences/ disabilities/ traumatic histories... just being a child or youth in a world that soaks them in comparison, materialism and overwhelming environments (school, for eg), worsened just by being online (no matter for 'healthy or unhealthy' reasons. Info overload=overwhelm.)
The children's questions: ' I feel unsafe/ uncomfortable/I don't fit in... what's wrong with me...?' are no longer met by trusted family/ friends.
The online search gives an answer.
One of my children was terrified by the answer... an awful, awful life sentence- if true. But a good soul, also so conflicted by wanting to be supportive of others in this position. And eventually when it arose in a teary midnight expose to me, I said 'that's all normal... you're not supposed to be interested in sex at 11! It's normal not to be interested in the materialistic image related garbage the girls in your class are into! Find the couple of kids who are interested in reading and science like you are!'
But society took this worry and fed it, to the degree I was called transphobic, ignorant and a bigot when I attempted to soothe.
So I said we'd get the gp to explain she was just a normal teenager with normal teen problems.
And that was the beginning of a journey I never foresaw, at that time.
6 years later, the loss of my business, home, work and marriage, to address the real underlying issues (which were neurodiversities and giftedness our entire, successful highly trained professional family members shared. )
Not out of the woods yet, but only focused on the life- enhancing routes to gear the kids to safe (SAFE) independent lives, which has meant I could not utilise public health, the normal pathways with gps and therapists, even the ndis. I couldn't let go around them joining groups like the local ladybird (autistic girls) social group. Which WorldCom would've been life changing in different circumstances.
So
Thank you.
I see now my intuition to avoid Headspace was very real. I shudder.
And I'm left with my vague question- who can compensate me for 10 years of my life (at least) lost and hundreds and thousands of dollars gone in income and on 'medical et al' expenses. Not to mention the rest.
And I would LOVE to support Jillian actively, as I have some of the skills and experience to be able to stand up with her. And you all. But I can't.
I can't risk losing what I've fought for, without their knowing, all these years, which is seeing my children go ahead and lead productive, happy and society- supporting lives.
Always
Thank you