
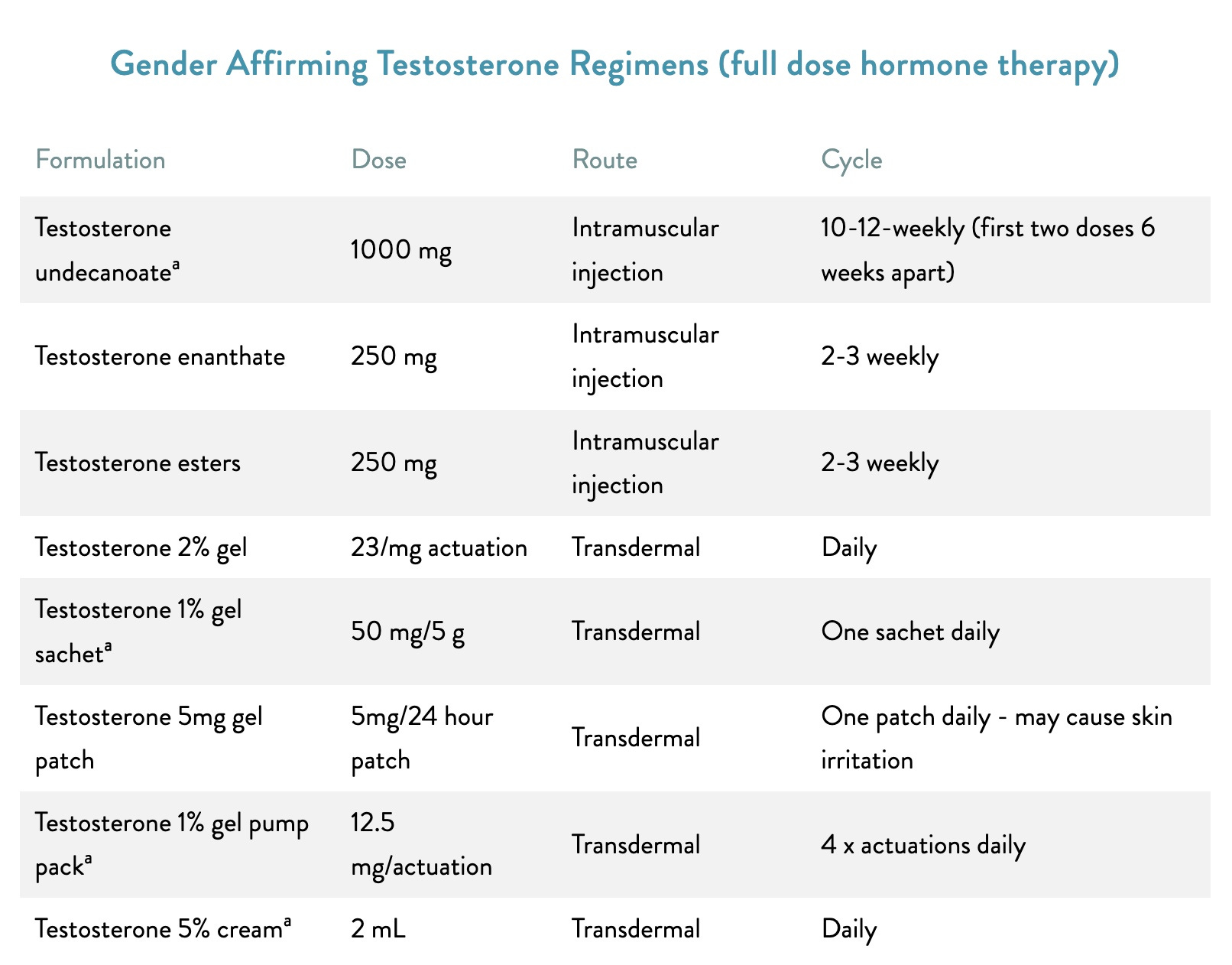
Testicle trouble
Male hormone shots for females with a 'testicular disorder'


Trans trend
A dramatic rise in taxpayer-funded testosterone for females is driven by a prescribing practice of questionable legality, according to University of Queensland emeritus professor of law Patrick Parkinson.
Transgender-identifying girls and women are being prescribed this masculinising hormone supposedly for the male condition “androgen deficiency due to an established testicular disorder.”
This diagnosis enables females who seek “gender-affirming” masculinisation as a transboy or transman to claim publicly funded testosterone under Australia’s Pharmaceutical Benefits Scheme (PBS). Subsidised testosterone is not available for gender dysphoria.1
“There’s real questions here about the legality of the prescription of testosterone to teenage girls—has it really been approved in accordance with the law?” Professor Parkinson said during a July 2 webinar with British paediatrician Hilary Cass.
“I’m not just asking the question—but the Health Department knows this, the Health Department has this data.”
In response to questions from GCN, the federal Department of Health reminded doctors that it is they who are to be held responsible.
“All aspects of patient care, including recommendations about appropriate treatments and the assessment of PBS eligibility are the responsibility of the treating doctor,” a departmental spokesman said.
In a 2019 Medical Journal of Australia (MJA) podcast, gender clinician and endocrinologist Ada Cheung said she had “checked this [prescription practice] with the PBS, they… have said that this is okay.”
She acknowledged there was no PBS listing for testosterone to treat gender dysphoria, but said “transgender men are males,2 and they have a low testosterone level, so they have androgen deficiency, and they don’t have testicles.”
Dr Cheung, who is a University of Melbourne researcher, was lead author of a “Position statement on the hormonal management of adult transgender and gender diverse individuals” published by the MJA in 2019.
That position statement says: “For [female] people requiring masculinising hormone therapy for gender dysphoria, we use the [PBS] authority indication ‘androgen deficiency due to an established testicular disorder’.”
“This [usage] acknowledges that prescribing gender-affirming hormones does not need to be based on a patient’s identity, but rather their physiology, which is accurate since bodies presumed female at birth3 don’t naturally produce enough testosterone on their own,” says the TransHub website run by ACON, a former gay rights organisation turned trans activist lobby.4
“Patients do not need to be registered with [Australia’s health insurance scheme] Medicare as male in order to access PBS-listed testosterone.”
Screenshot: TransHub on the ways and means of testosterone as a cross-sex hormone
Androgen desexed
In 2015, the advocacy group now known as LGBTIQ+ Health Australia successfully lobbied for removal of the requirement that androgen deficient patients given PBS testosterone be male.5
There was no discussion of the health risks for females exposed to testosterone in the “public summary document” from the relevant July 2015 meeting of the Pharmaceutical Benefits Advisory Committee, the independent expert body which recommended that the health minister de-sex the PBS listing.
Last month, Australia’s Liberal Party Senator Claire Chandler released departmental data showing that 6,559 patients recorded as female were dispensed testosterone in 2023 for the PBS condition androgen deficiency involving a testicular disorder.
This all-age total represented a 140 per cent increase since 2019.
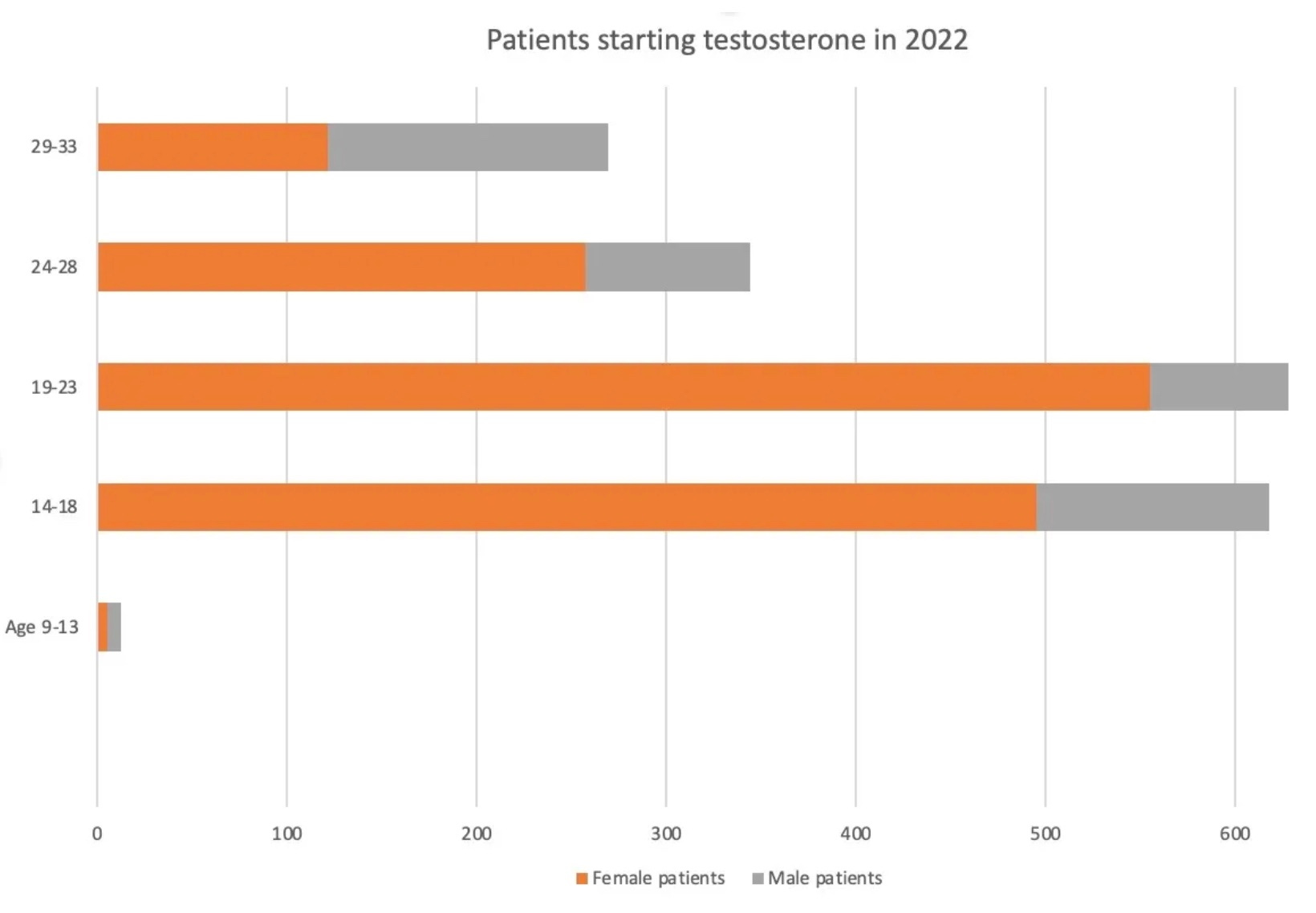
Last November, GCN reported that an estimated 1,433 females under the age of 34 started PBS-funded testosterone for androgen deficiency in 2022, almost 1,000 more than the number of males, who would indeed suffer from low levels of natural testosterone.
Chart: Young women and girls overtake males as new patients starting PBS-funded testosterone for androgen deficiency involving a testicular disorder
Future reckoning
“There are huge ethical and legal concerns with doctors claiming that girls and young women have testicles in order to attract a taxpayer subsidy for ‘gender-affirming’ testosterone,” Senator Chandler told GCN earlier this month.
“PBS-subsidised testosterone being prescribed by doctors declaring it is to treat a medical condition—despite knowing full well it is being sought for ‘gender affirmation’—should be a major concern to health authorities, yet they have turned a blind eye.
“We know that giving girls and young women testosterone can lead to serious, irreversible effects.6 When young women are inevitably seeking answers about what was done to them in the years ahead, I hope the doctors involved are prepared to explain before a court why they claimed that these women had a testicular condition.”
Video: British trans influencer Noah on the vagaries of testosterone
Binary rules
At the July 2 Cass webinar, Professor Parkinson also questioned the legality of testosterone given to “non-binary” adolescents.
“The Family Court hasn’t endorsed this,” he said.
He said that in approving cross-sex hormone treatment, the court acted on the binary assumption that “the treatment would be to bring a male into a female presentation or female into male—but it must be, according to the High Court of Australia, the treatment of a disorder or illness of some kind.”7
“So, we’re seeing medical treatments given to ‘non-binary’ teenagers. There is no presentation of what it means to be non-binary, anatomically, to which they can be helped to transition—in my view, it is unlawful and unethical.”
He said he believed there were at least two gender clinics run by state health departments where “non-binary treatments are being offered as a kind of cosmetic treatment [for adolescents].”
After the webinar, Professor Parkinson told GCN that he was not aware of any medical evidence “that supports what are in effect cosmetic modifications desired by a young person as a treatment for gender dysphoria.”
In a 2021 podcast, Australia’s best known gender clinician, Michelle Telfer, said that her clinic at the Royal Children’s Hospital (RCH) Melbourne was witnessing more young people seeking “further individualisation of hormone treatment.”
“This has really come from demand from the [trans] community and listening to what the trans community are telling us in terms of what they need,” Dr Telfer said.
She gave the example of a female who identified as “non-binary” and might only want six months of masculinisation on testosterone. (A female identifying as male would be expected to take lifelong hormones.)
“We’re seeing more and more young people coming to us with that idea that they don’t want the full gamut of puberty blockers, gender-affirming hormones and then surgical treatment—they might want a little bit of that,” said Dr Telfer, who at the time was director of the RCH Melbourne gender clinic.
GCN put questions to RCH Melbourne and Drs Cheung and Telfer. GCN does not dispute that gender-affirming clinicians believe their interventions help vulnerable youth
Hormonal treatment of gender dysphoria is “off label”, meaning it does not have regulatory approval for that condition.
By definition, a transman is female.
“Presumed female at birth” is an activist term for a girl or woman but with the suggestion that the observation of a child’s sex is erratic.
ACON has a seat on the LGBTIQA+ Health and Wellbeing 10 Year National Action Plan Expert Advisory Group chaired by Australia’s Assistant Minister for Health, Ged Kearney.
LGBTIQ+ Health Australia is also represented on the LGBTIQA+ Health and Wellbeing 10 Year National Action Plan Expert Advisory Group.
The risks of testosterone taken to “masculinise” a female include sterilisation, sexual dysfunction and cardiovascular problems.
In a 2022 journal article, Professor Parkinson noted that the High Court in the re Marion case had held “that parents do not have the legal authority to consent to a sterilisation operation on their child, otherwise than as an incidental result of surgery performed to cure a disease or to correct a physical malfunction.” This reasoning was applied to gender dysphoria cases in the Family Court, whose 2017 re Kelvin decision ended the requirement for judicial authorisation before a minor could begin cross-sex hormone treatment with the risk of sterilisation. The court majority, relying on evidence from the RCH Melbourne gender clinic, found that the science of gender dysphoria had advanced, and the therapeutic benefits of the hormone treatment outweighed the risks. This re Kelvin ruling has come in for heavy criticism.
It is surprising that those promoting and implementing the affirmative model of ‘gender care’ seem not bothered by the fact that it has no acceptable ‘evidence base’, the requirement to confirm efficacy and safety of an invasive, irreversible and sterilising procedure (all the more important when children are involved).
There can be a high price to pay for ignoring that requirement. I cite a case in point:
In 1998 the ‘Pelvic Mesh Sling’ (a device invented in the 1980’s by Australian urogynaecologist Dr Peter Petros ) was for the first time
surgically implanted in the pelvis of women who experienced ‘pelvic-floor dysfunction’, a not uncommon disabling problem following childbirth.
The device had not undergone an appropriate clinical trial and its use was not ‘evidence based’. Regardless, the TGA approved the device in 2003 and the Australian Medical Association (AMA) became the exclusive distributor for the device.
Around 100,000 women in Australia were thus treated; however, within a few years problems surfaced.
The mesh tended to migrate and perforated organs including the bladder, urethra, vagina and bowel, resulting in severe pelvic pain, dyspareunia, organ dysfunction, systemic autoimmune conditions and urinary incontinence.
Many women required multiple surgeries in an attempt to remove mesh fragments and use of the device was banned in 2018 by the ‘Medical Device Regulator’ (a part of the TGA that had initially approved the device).
Multiple legal suits, amounting to billions of dollars, followed and thousands women were left permanently damaged.
The intervention was not evidence based, the AMA and TGA got it horribly wrong.
. . . . . However, we are reassured that treating a cohort of children, known to be heavily burdened with a range of mental health conditions, with gender blockers, cross-sex hormones and irreversible sterilising genital and breast surgery does not require an evidence base.
. . . . Evidence aside, we are reassured that ‘lives are being saved’.
1 Dr Peter Pedros was deregistered for professional misconduct in 2019
This is consistent with my observation:
The origin and continued propagation of trans is via Psychiatry. Not media, not queer studies, not politics, not trans, not social media or the internet, and not postmodernism.
It is Psychiatry at a medieval level totally lacking in science, the kind of psychiatry which works with demonic possession and trepanning skulls.
Because of this it is the single psychiatric condition requiring surgical removal of healthy tissue for “treatment”, and the only psychiatric condition requiring the rest of world to conform to a patient’s delusion.
All this would vanish if doctors simply said it is a delusion, which it is. But then 100+ years of “science” is thrown into doubt. The only recourse is legislation.