


Take care
Psychiatry college acknowledges some tough realities of detransition

Be warned
Psychiatrists in Australia and New Zealand have been put on notice that detransitioners may feel harmed by “gender-affirming” medicine, that some have launched lawsuits and that the true rate of treatment regret is unknown.
This new warning appears in an updated position statement on the hot button topic of gender dysphoria issued this week by the Royal Australian and New Zealand College of Psychiatrists (RANZCP), without any publicity.
The document, which blends gender ideological jargon with a defence of traditional comprehensive assessment and formulation, also recognises that some former patients conclude their dysphoria was due to other, non-gender issues such as trauma, internalised homophobia and mental health problems.
“It is not known how many individuals who detransition experience regret, and how many are satisfied with the changes they have made,” the RANZCP statement says. “While regret appears to be infrequent, the true regret rate is unclear.”
Gender-affirming activists seek to minimise the significance of detransition, which undermines the dogma that even young children and teenagers are “experts” in “gender identities” untethered from birth sex.
In a 2021 journal debate over the extent of transition regret, researcher Dr Ken Pang, from the gender clinic at the Royal Children’s Hospital (RCH) Melbourne, and colleagues said “the only relevant case of regret of which we are aware is Keira Bell [the detransitioner who took the London-based Tavistock clinic to court], although presumably there are others.”
Against this background, the RANZCP’s acknowledgment of the plight of detransitioners—and its account of their depression, anxiety and difficulty in getting help—is seen as a positive step by sceptics of the gender-affirming worldview.
“It is welcome to see the college officially recognise the phenomena of regret and detransition; the harm that this has caused and the associated risk of medical malpractice litigation; and the special need for dedicated services for this group [of detransitioners] now and in the future,” a senior psychiatrist, speaking anonymously to avoid activist harassment, told GCN.
Sydney psychiatrist Dr Patrick Toohey has been sued in the NSW Supreme Court by a regretful detransitioner, Jay Langadinos; the case is in its early stages. At least one potential test case involving disputed access to gender medicine for a minor has been settled in Australia’s Family Court. There is speculation about a class action being launched, although this is seen as a difficult exercise.
“I think this is a radical position statement [from the RANZCP]— to come out boldly to say that ‘sex refers to the biological characteristics that define humans as female or male’, at the very time when politicians in [Australian] Senate hearings are being asked to define what is a woman and they can’t.—Psychiatrist Dr George Halasz, interview with GCN, 13 December 2023
Pushback
The new RANZCP statement follows an early review under pressure from the gender-affirming lobby unhappy with the college’s first considered and cautious position statement on gender dysphoria adopted as recently as September 2021. In a letter to the college two months later, a group of transgender lobbies lodged various objections, including that the use of the term “co-morbitity implies that being trans is a disorder.”
The 2021 RANZCP statement has been cited internationally as one among other proofs of greater caution over gender medicalisation.
The just-updated 2023 version is “a vast improvement on the previous iteration”, according to a message to members of the Australian Profession Association for Trans Health (AusPATH), which functions as a gender-affirming lobby group. The message did not explain the nature of this improvement, and AusPATH did not reply to GCN’s request for comment.
Although the 2023 statement seeks to present trans identity as depathologised and attributes the associated mental health problems to a discriminatory society, the document acknowledges divided expert opinion on gender dysphoria and does not embrace an affirmation-only approach.
“Professional opinions differ about some aspects of the most appropriate care for adolescents requesting treatment,” the new statement says. “A range of interventions (including psychological, social, and medical) may be considered for adolescents presenting with distress related to their gender.”
An Australian child and adolescent psychiatrist, Dr Jillian Spencer, has been stood down from clinical duties at a children’s hospital following a complaint of “transphobia” and her attempts over many months to raise concerns about the possible harm done by the hospital-imposed monopoly for the contested gender-affirming treatment approach.
In its new position statement, the RANZCP notes that “psychiatric practice will be informed by further emerging evidence” but did not reply when GCN asked how often the statement would be revisited for an update.
The college’s first gesture of caution came in September 2019 when it deleted, without announcement, its explicit endorsement of the confident gender-affirming treatment guideline issued the year before by the RCH gender clinic. This followed critical coverage of the RCH guideline in The Australian newspaper (Disclosure: I was the journalist—BL).
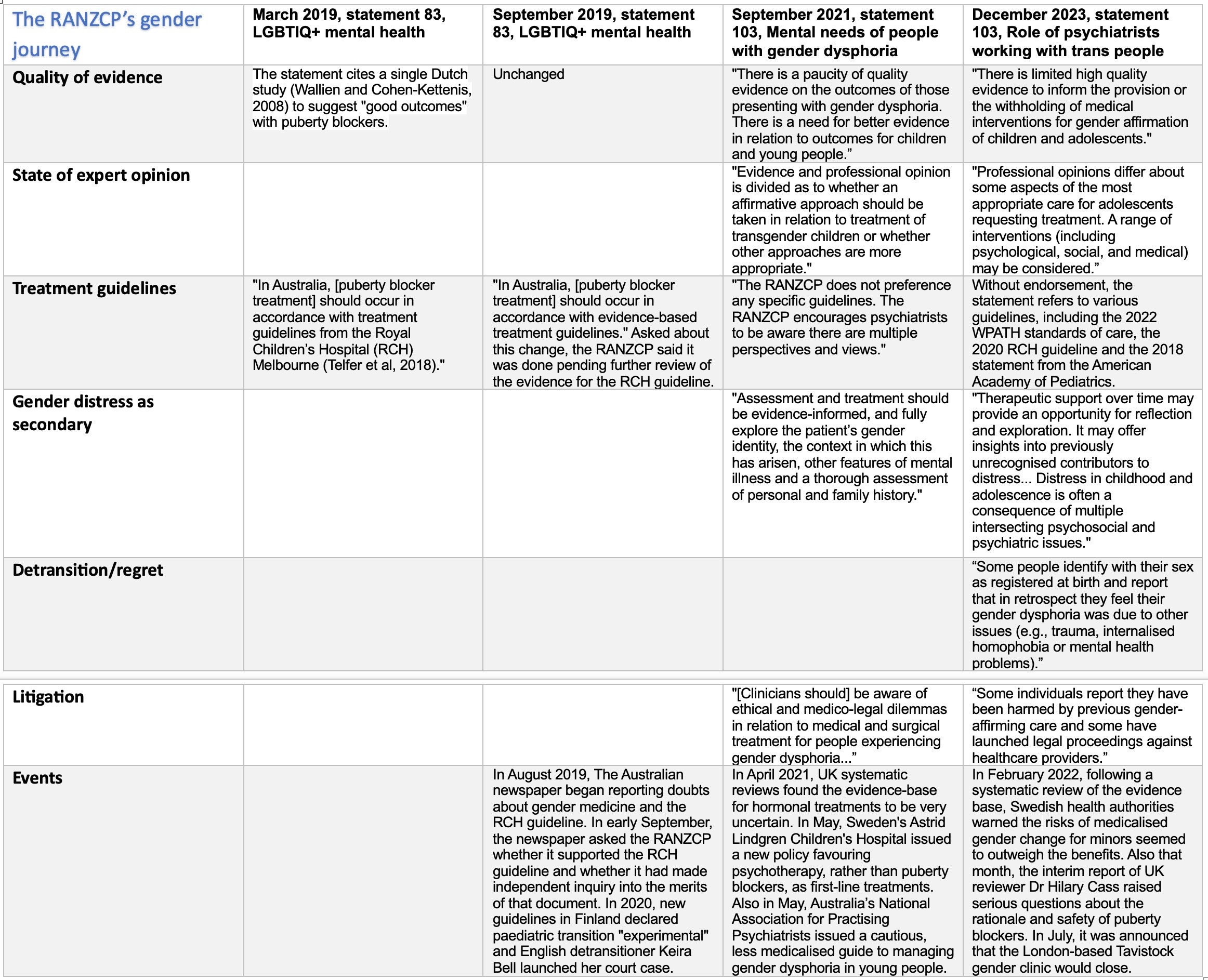
Chart: Since 2019 the RANZCP has elaborated a more detailed and cautious position on gender dysphoria
A glimpse of Europe
The 2023 RANZCP statement updates psychiatrists with Europe’s post-2019 shift to caution on gender medicine, although the reference is fleeting and vague.
“While a number of major professional organisations support the use of puberty suppressants and cross-sex hormones for adolescents, health authorities in some European countries have recommended restrictions be placed on their use,” the document says. “Australian and New Zealand paediatric services continue to provide multidisciplinary gender-affirming care [including puberty blockers].”
The college’s account underplays the systematic reviews of the evidence base commissioned in Finland, Sweden and England, the characterisation of puberty blockers as experimental, and the importance of England’s independent review of dysphoria care under paediatrician Dr Hilary Cass.
Psychiatrist Dr Roberto D’Angelo, president of the Society for Evidence-based Gender Medicine, which scrutinises the dogmatic claims of the gender-affirming lobby, said he believed the college’s new statement was “an improvement” on the 2021 version. He served on the steering group for the 2023 statement but spoke with GCN in a personal capacity.
“However, I think [the new document] still minimises the significance of the outcomes of systematic reviews and the findings of the low-quality evidence base,” he said. “And it also does not capture the significance of the changes in Europe.”
Although the RANZCP statement does reference Dr Cass’s 2022 interim report, it does not pick up its warning about the trend to “socially transition” young children, whereby adults enable them to live out an opposite-sex role.
One psychiatrist pointed out to GCN that the statement pushed the use of pronouns and upheld the taboo against “misgendering” but failed to “acknowledge the Cass review finding that social affirmation is a powerful psychosocial intervention that increases the likelihood of the individual progressing to medical affirmation.”
The college does not address the contradiction between puberty blockers being still available as routine treatment in Australia and New Zealand while this treatment is regarded by European health authorities as so poorly evidenced that it should be largely confined to strict clinical trials.
At one point, the new RANZCP statement says there is “limited high-quality evidence to inform the provision or the withholding of medical interventions for gender affirmation of children and adolescents.”
Dr D’Angelo said he believed this claim was “misleading and factually incorrect [because] all systematic reviews have found that there is no high-quality evidence.”
“Whilst the position statement highlights the importance of informed consent, an accurate explanation of the quality of the evidence base is crucial for informed consent. I am concerned that clinicians and parents may be given a falsely positive impression of how strong this evidence is.”
“The two most experienced clinicians involved in transgender healthcare in Ireland have made a formal complaint to the Health Information and Quality Authority (HIQA) about the [public] Health Service Executive’s (HSE) treatment of children with gender identity issues. Professor Donal O’Shea and psychiatrist Dr Paul Moran of the National Gender Service allege the HSE has been directing children to services overseas that adhere to a so-called ‘gender-affirming’ model of care. Prof O’Shea and Dr Moran say the gender-affirming model can damage children and is associated with a greater readiness to start on inappropriate medical treatment for patients presenting with gender identity issues. Dr Moran [said] the complaint to HIQA cited ‘a series of cases as examples of harm and risk caused to Irish children by these services’.”—news report, RTÉ Prime Time, Ireland, 14 December 2023
Video: Prime Time, the flagship current affairs program of Ireland’s public broadcaster RTÉ, scrutinises the ideological gender-affirming treatment approach
Psychotherapy stays
The college has held the line against the gender-affirming campaign to frame exploratory psychotherapy as an unethical practice that seeks to change or suppress a young person’s gender identity. Australia’s state of Tasmania is the latest jurisdiction pushing for adoption of a new criminal law which would exempt medicalised gender change from prosecution as “conversion therapy”.
“Psychotherapy is not conversion therapy,” the RANZCP statement says. “In psychotherapy, the patient’s autonomy and self-determination is respected and the therapist does not impose predetermined notions of gender or sexual orientation on the patient.”
“Therapeutic support over time [for a trans-identified person] may provide an opportunity for reflection and exploration. It may offer insights into previously unrecognised contributors to distress, depending on the individual person.”
Dr Philip Morris, president of Australia’s National Association of Practising Psychiatrists, which adopted a cautious policy on youth gender dysphoria before the RANZCP, welcomed the college’s stout defence of psychotherapy.
Dr Morris said the new RANZCP statement “takes into account the complexity and nuance of the treatment of kids”, unlike the college’s radical March 2019 policy which simply directed psychiatrists to the “very affirmative” and medicalised 2018 treatment guideline from the gender clinic of the Royal Children’s Hospital Melbourne.
Citing gender clinic waiting lists, the gender-affirming lobby is pushing for more family doctors (known as general practitioners or GPs) to start 16- and 17-year-olds on irreversible cross-sex hormones.
Dr Morris said the RANZCP’s 2023 document acknowledged the legitimate role of “psychological therapy, not just as psychological therapy for supporting a person going through medical transition, [but] as an alternative to medical affirmation.”
“[The statement] acknowledges there are situations where gender dysphoria is, in a sense, the tip of the iceberg of an underlying condition, so it acknowledges that differential diagnosis needs to be undertaken.”
Dr Morris noted that the statement had not embraced the “affirmation-only” worldview of gender-affirming activists but rather had recognised that “the evidence base is still very weak—that there’s not enough evidence for the college to recommend a particular approach.”
“Have you detransitioned? You may be eligible to volunteer for a 35-45-minute survey and optional 60-70-minute follow-up research interview if you are aged 16 or older [and] live in Canada or the US… We are interested in hearing from a wide range of people who detransitioned whether it was because you had medical complications from transitioning, because your identity changed, or you were misdiagnosed, you lost access to healthcare, or any other reason.”—Recruitment material for a new study, Detransition Analysis, Representation and Exploration (DARE), December 2023
Young and different
Veteran Melbourne child psychiatrist Dr George Halasz, who serves on the editorial committee of the journal Australasian Psychiatry, welcomed the statement’s endorsement of “developmentally responsive care.”
The college’s statement says: “Childhood and adolescence are times of rapid and dynamic brain development and development of personal identity.
“Further, distress in childhood and adolescence is often a consequence of multiple intersecting psychosocial and psychiatric issues. As a result, the clinical care and assessment of [trans and gender-diverse] children and adolescents can be complex.”
Dr Halasz told GCN he believed the new RANZCP statement confirmed “a fundamental shift away from the strict adherence to the affirmative model”, which in his view “distorts the [developmental realities of the young] into something unrecognisable—that a child’s wish becomes the clinician’s order or command.”
“The mind and the brain in the context of a child and an adolescent are different fundamentally from the mind, context and make-up of an adult, where autonomy is assumed—it cannot and must not be assumed in a child.”
Dr Halasz said he agreed with the college statement’s reassurance that “gender expansive and non-conforming behaviour and preferences can be normal at any age and should not necessarily be a cause for concern or require attention.”
But he said this raised an unanswered question—“What’s the defence of the affirmative model which on hearing [of gender non-conforming behaviour], affirms it, rather than assesses it as normal? Because once it’s affirmed, you’re on a pathway [to medicalisation with a locked-in gender identity].”
“[In this study] youths with a history of mental health issues were especially likely to have taken steps to socially and medically transition. This relationship held even after statistically adjusting for likely confounders (e.g., age). The finding is concerning because youth with mental health issues may be especially likely to lack judgment necessary to make these important, and in the case of medical transition permanent, decisions. The finding supports the worries of parents whose preferences differ from their gender dysphoric children. It is consistent with another finding of this study, that parents believed gender clinicians and clinics pressured the families toward transition. The finding is particularly concerning given that parents tended to rate their children as worse off after transition.”—A study of parent reports on 1,655 possible cases of rapid-onset gender dysphoria, Diaz et al, Journal of Open Inquiry in the Behavioral Sciences, October 2023
Wrong diagnosis
Another experienced psychiatrist, who spoke anonymously to GCN in order to protect his livelihood from activist attack, predicted there would be “pushback from the usual suspects because [the new RANZCP statement is] not entirely fawning and one-sided about gender affirmation.”
However, he highlighted wordy and contradictory elements in the document, reflecting the struggle between partisans and sceptics of the gender-affirming way.
“It’s full of motherhood statements, and it looks like it’s been stuck together by committee. It’s not a coherent document,” he said.
This psychiatrist felt the profession was unwilling to confront the mistaken nature of the gender dysphoria diagnosis, and too often went along with the ideological assumption that mental health “co-morbidities” were products of a “transphobic” environment.
“I’ve always viewed this whole diagnosis [of gender dysphoria] to be one of dubious validity. And I’ve always seen it to be part of an underlying personality disorder, either emerging or already in existence, with very strong social and familial and cultural determinants.”
He said many psychiatrists recognised borderline personality disorder, for example, among troubled adult patients presenting as gender dysphoric, but feared to acknowledge this openly because the field had become so politicised.
He said it was contentious to diagnose personality disorders in children and adolescents who were still undergoing identity formation.
However, he believed gender confusion in young children would often be “driven by gender ideology in one or both parents”—and encouraged by gender-neutral social engineering.
Within a family, he said, the contested gender identity of a child “can be leveraged as a weapon in an interpersonal dispute between married, separated or divorced parents.”
“The closer an adolescent is to adulthood, the more likely it is that what is presented as gender dysphoria is secondary to a personality disorder,” he said.
“The lack of credible evidence of benefits of gender transition has come into focus for today’s transgender-identified youth, whose numbers have sharply increased. The presentation of gender dysphoria has markedly changed in recent years: the sex ratio of youth presenting in medical settings has reversed from primarily male to primarily female, with the preponderance of youth whose transgender identity emerged for the first time in adolescence and in the context of significant pre-existing mental illness and neurocognitive disorders. These changes began to manifest around 2006 but became pronounced around 2014–2015. Nonetheless, many clinicians and policymakers promulgate that science long ago established the benefits of gender transition for these adolescents.”—journal article, Prof Stephen B Levine and E Abbruzzese, Current Sexual Health Reports, April 2023
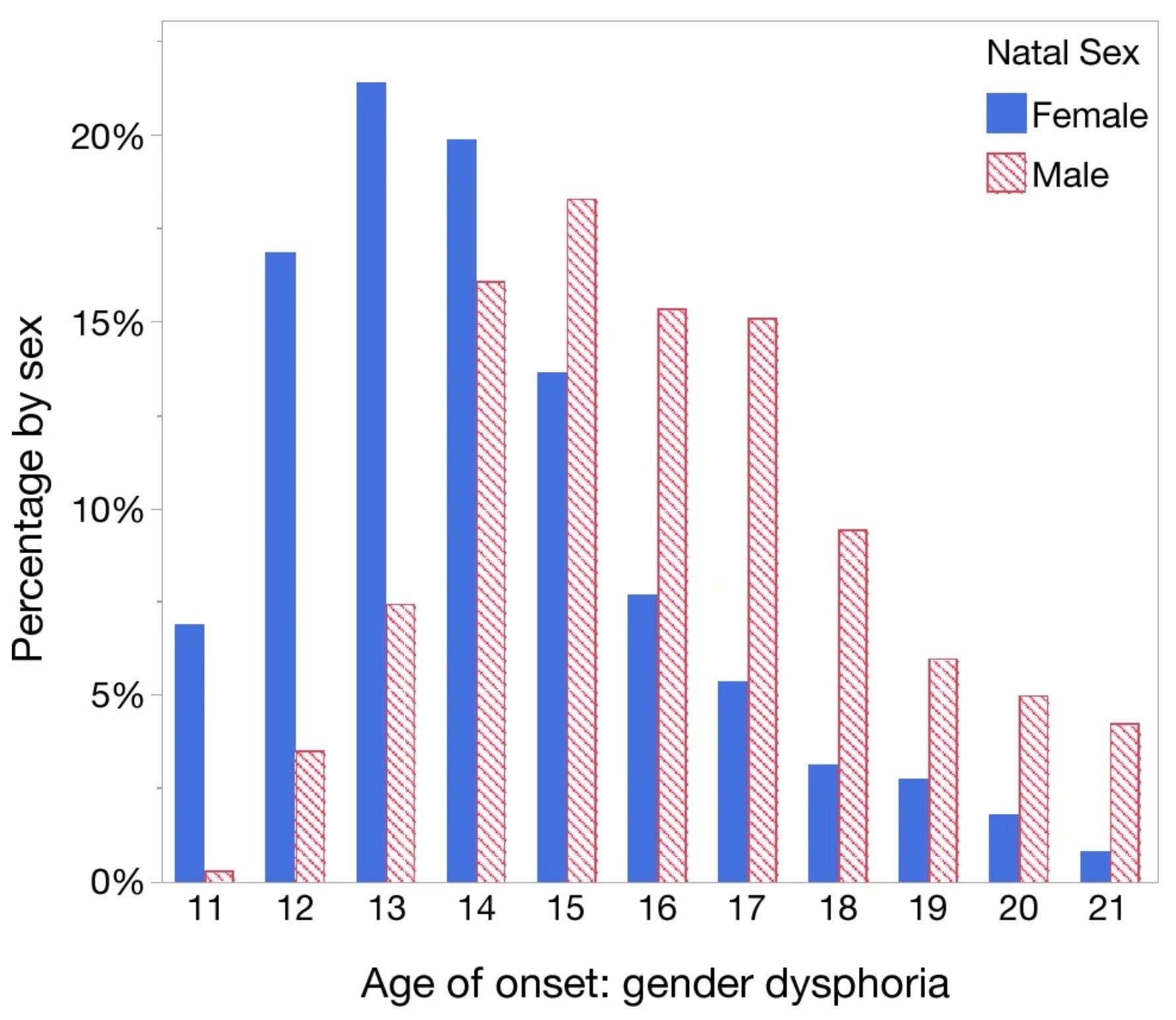
Chart: The spread of age of onset of gender dysphoria in a group of males and females in a study relying on reports from parents
The patient flip
The new RANZCP statement devotes separate sections to adults on the one hand, and children and adolescents on the other.
However, the document is silent on a central reason for concern about medicalised gender change—the explosive growth internationally of atypical cases of gender dysphoria chiefly among teenage females. The condition used to be rare and mostly confined to boys, with onset in early childhood. This flip in patient profile was hinted at in the college’s 2021 statement.
The updated 2023 document also fails to address the related debate about the possible role of social contagion of trans and non-binary identities online and through peer groups.
However, psychosocial influences on gender distress does get a mention in the new statement, and there is a reference to a 2021 detransition study by American researcher Dr Lisa Littman, who is persona non grata among affirmative activists because of her hypothesis of rapid-onset gender dysphoria spread by social contagion.
The RANZCP statement does not enumerate the risks of harm—risks acknowledged by some gender-affirming clinicians—that come with puberty blockers and cross-sex hormones, including sterilisation (“reduced fertility” is mentioned), sexual dysfunction and cardiovascular disease.
GCN does not dispute that gender-affirming clinicians genuinely believe their interventions help vulnerable youth. Comment was sought from the RANZCP, AusPATH and RCH.
I note that you talk frequently about "medicalized gender change", both here and in your recent "Doctors disagree" post:
https://www.genderclinicnews.com/p/doctors-disagree
Which I suppose is a step in the right direction away from the rather unscientific and quite odious "sex change" euphemism which too many throw about with gay abandon, so to speak:
https://christopherrufo.com/p/sex-change-procedures-at-texas-childrens/comment/16193243
However, even "medicalized gender change" seems a rather odious euphemism in itself, particularly when the upshot is to sterilize autistic and dysphoric children, to turn them into sexless eunuchs. At least according to the standard biological definitions for the sexes promulgated in reputable biological journals, encyclopedias, and dictionaries:
https://academic.oup.com/molehr/article/20/12/1161/1062990 (see the Glossary)
https://link.springer.com/referenceworkentry/10.1007/978-3-319-16999-6_3063-1
https://web.archive.org/web/20181020204521/https://en.oxforddictionaries.com/definition/female
https://web.archive.org/web/20190608135422/https://en.oxforddictionaries.com/definition/male
https://twitter.com/pwkilleen/status/1039879009407037441 (Oxford Dictionary of Biology)
And:
"What are biological sexes?":
https://philarchive.org/rec/GRIWAB-2
Wiley Online Library [WOL]:
"Biological sex is binary, even though there is a rainbow of sex roles"
https://onlinelibrary.wiley.com/doi/epdf/10.1002/bies.202200173
Basically, by those quite standard and well-regarded biological definitions, to have a sex is to have functional gonads of either of two types, those with neither being, ipso facto, sexless. Hence the justification for saying that the transgendered who have had their gonads removed are now sexless eunuchs. Fine, I guess, if adults want to do that to themselves, but it has to qualify as an absolutely monstrous crime to trick dysphoric children into thinking such "gender affirmation surgeries" are, in any way, equivalent to changing their sex.
So it is hard not to see that phrase -- "medicalized gender change" -- as little short of equally odious euphemisms like "ethnic cleansing", like "final solutions". It makes "sense" to take kids with some "gender non-conforming" or sex-atypical personality or behavioural traits and mangle their genitalia into some ersatz replicas of those of the other sex?
"monstrous" doesn't begin to describe that crime, that medical scandal of the centuries. Some "doctors" -- despite what they "genuinely believe" -- deserve to lose their licenses if not be strung up by their nuts and left to twist in the wind. A recent post by Denton Yoga-Carter aptly titled "Words" has a short compendium of images, of graphics that sort of summarizes that rather odious state of affairs, but a particularly arresting, and quite damning one says:
"Start Thinking of an Excuse Why You Supported Sterilizing Children"
https://dentonyogacarter.substack.com/p/words
it is interesting to reflect on a statement issued by the Royal Australasian College of Physicians (RACP) on 6th March 2020:
"The RACP strongly supports expert clinical care that is non-judgmental, supportive and welcoming for children, adolescents and their families experiencing gender dysphoria. Withholding or limiting access to care and treatment would be unethical and would have serious impacts on the health and wellbeing of young people.
Most significantly, we applaud the College’s stance in validating the work of Associate Professor Michelle Telfer and her colleagues nationally by calling on the Government to work with these experts to develop evidence-based fact sheets for patients and families".
A basic tenet in the practice of medicine is that new therapies/ interventions must be tested to confirm safety and efficacy. The ‘test’ consists an appropriate clinical trial.
Obviously an intervention as extreme as one undertaken in children and young people that is invasive, mutilating, irreversible and sterilising demands the most rigorous test/trial available.
No such test/trial in the affirmative management of Gender Dysphoria has been undertaken anywhere in world!
At this time, some near four years after the statement quoted above, I suspect that the RACP would be reluctant to provide such a ringing endorsement of the affirmative management protocol of gender dysphoria as practices by Melbourne's RCH, given the doubts raised by respected authorities and institutions given doubts as to the efficacy and safety of that approach.