
Off the trans train
Child and adolescent psychiatrist Sven Roman explains Sweden's historic turn towards caution on gender medicine


Young people with immature brains cannot grasp the consequences of irreversible gender medicalisation, a prominent Swedish child and adolescent psychiatrist has warned.
“It is my opinion that the irreversible measure of sterilisation should not be carried out until the age of 25, and it is therefore appropriate to have the same age limit for gender-reassignment treatment for gender dysphoria,” the psychiatrist, Dr Sven Roman said.
“[In the adolescent brain, the] frontal lobe matures last, at 25-30 years of age. This is where overall thinking and judgment are located. A teenager can therefore not understand the consequences of an irreversible sex-change treatment.”
Dr Roman, who trained in medicine at the prestigious Karolinska Institute, said he believed that social contagion in the age of smartphones and social media “largely explained” Sweden’s “astonishing” surge in atypical cases of gender dysphoria chiefly diagnosed among adolescent females.1
He made the remarks in an expert report for the American Supreme Court test case, US v Skrmetti, which involves a constitutional challenge to Tennessee’s law prohibiting gender medicalisation of minors. Hearings may begin later this year.
Dr Roman said he had taken part in about 600-700 neuropsychiatric investigations and evaluations and in the course of his work, had met about 30 children with diagnosed or self-identified gender dysphoria. His opinion on the issue was also shaped by his study of the international scientific literature.
While the evidence for puberty blockers and cross-sex hormones was “non-existent or extremely weak”, there did exist evidence-based treatments for co-morbidities common among these young people, such as depression, anxiety, autism and ADHD, he said.2
And he said non-invasive treatment of those co-morbid conditions was known to “resolve gender dysphoria in many such cases.”
“It is my experience and the opinion of many psychiatrists in Sweden that psychosocial treatment of gender dysphoria for children and young adults should always be tried first [before any talk of medical intervention],” Dr Roman said.
After concerned experts kick-started public debate in Sweden in 2019, a systematic review of the evidence for paediatric gender medicine was undertaken, leading Sweden’s National Board of Health and Welfare to issue new, more cautious treatment guidelines in 2022, representing “essentially a ban on puberty blockers, cross-sex hormones, and surgeries in children,” Dr Roman said.
He said the new policy, comparable to the position adopted by England’s National Health Service after the 2020-24 Cass review, left open the possibility of medicalised gender transition in exceptional cases3 and in research.
“In revising its recommendations, the National Board of Health and Welfare has taken account of the fact that the efficacy and safety, benefits and risks of [hormonal] treatments are not proven and that three factors have shifted the balance between benefit and risk in a negative direction [one factor being the phenomenon of detransition of former patients reported in 2021 studies by American physician and researcher Dr Lisa Littman and detransitioner Ellie Vandenbussche].”—Sweden’s National Board of Health and Welfare, summary of new more cautious national guidelines, December 2022
Learning and behaviour
In his expert report, dated May 2023, Dr Roman said social transmission of psychiatric syndromes was “very common,” especially among teenage and young adult females. He cited the examples of anorexia being reinforced among groups of in-patient females, and the practice of sharing images of self-harm on social media.
He said the incidence of gender dysphoria in Sweden took off as more teenagers got smartphones after 2007 and as offline contact among many teenage girls gave way to online-only contact since the 2010s.4
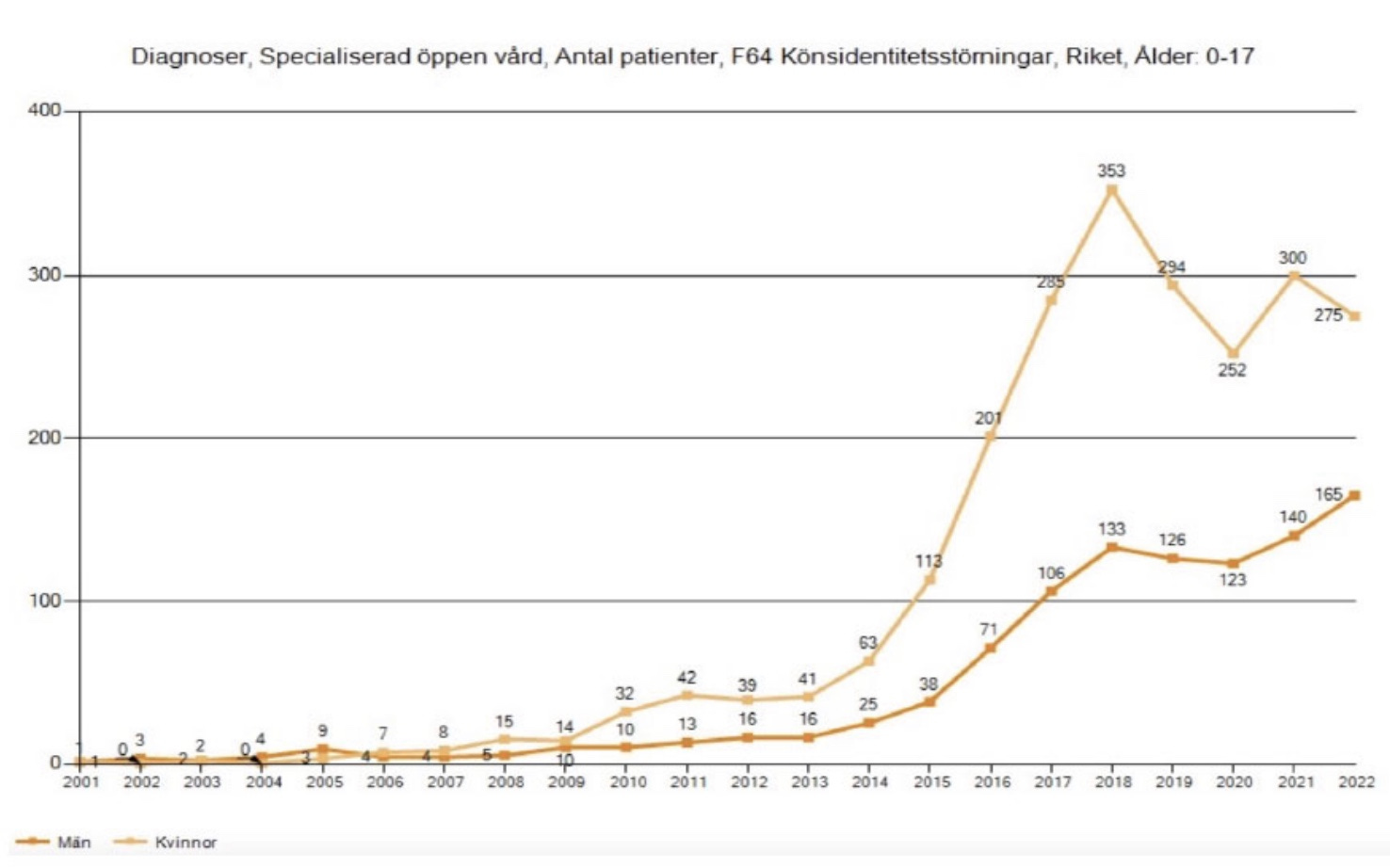
“The increase in the diagnosis of childhood gender dysphoria was moderate until 2007, the year the iPhone was introduced… and then the increase accelerated to become very high from 2014 onwards, when social media had become ubiquitous among adolescents,” he said.
“The fact that gender dysphoria is socially contagious is also illustrated by the fact that the gender dysphoria diagnosis among children in Sweden decreased in 2019 and 2020, when the public debate [involving concerned experts and parents] was initiated,” he said.
“But when Sweden from spring 2020 to 2021 had restrictions due to the Covid-19 pandemic, including distance learning in upper secondary schools and universities and less incidence of organised sport, many teenagers and young adults became socially isolated and then the trend reversed and the number of gender dysphoria diagnoses for children increasing again.”
Chart: The number of cases of “gender identity disorder” (an earlier form of the diagnosis of gender dysphoria), nationwide in Sweden for females (the steeper line, especially after 2014) and males aged under 18
Medicalising an identity crisis
Through his involvement with the parents’ group GENID, Dr Roman said he had learned “that children frequently desist5 from their gender dysphoria when they receive psychotherapy or other interventions to address psychiatric comorbidities.”
“Teenagers routinely experience mild body dysmorphia (unhappiness with their physical appearance) and sometimes psychotherapy and the maturation process are all a child needs to resolve what the child may call gender dysphoria.”
Dr Roman quoted a colleague Professor Mikael Landén, a leading psychiatrist, an author of Sweden’s systematic review and a clinician who had been treating patients with gender dysphoria since the early 2000s.6
In objecting to a 2018 proposal by the Swedish government to allow legal gender change for children from the age of 12, Professor Landén said: “Exploring different identities as a teenager is a natural developmental step towards adulthood.”
“Identity formation options vary with the zeitgeist. While young people in the eighties wondered whether they were a synthesiser or a punk, young people today are asked to consider whether they are male or female.
“Even though this is not a real choice—gender is natural—some young people will still experiment with gender expression and explore what applies to them, [this is] what is known as an identity crisis.
“Personal identity is formed in several stages and reassessed over time. The search for identity is not a single irreversible event. We don’t see many 55-year-old punks on the streets, even though their identification was very strong when they were young.
“Changing legal gender during what may be a temporary identity crisis risks putting [young] people on an irreversible path towards medical treatments that can lead to sterility and bodily harm,” Professor Landén said.7
“I do have something (indeed, quite a lot) to say about what I consider to be possibly one of the (perhaps the) greatest scandals in medical history… about the absolutely horrendous situation in Sweden where in a population of 10 million people—about 2 million of whom are children under the age of 18—some hundreds of children per year are now given puberty blockers etc. (which will make them sterile) and many of them receive this ‘treatment’ in the face of their parents’ doubts and refusal to go along with the whole thing.”—Child and adolescent psychiatrist, Professor Christopher Gillberg of Gothenburg University, Sweden, email to Bernard Lane for news report in The Australian, 18 September 2020
“I have worked clinically and in research in child psychiatry/child health for 45 years and have ‘always’ seen a very few cases per decade with transsexualism with onset under age five years. Virtually all the new cases occur in adolescents who did not show any ‘trans-tendencies’ before age 10. Many of the Swedish [rapid-onset gender dysphoria] cases have autism or anorexia nervosa.
“In my experience, it is extremely common for individuals with these conditions to have even more ‘identity problems’ in puberty (‘who am I, how should I behave, what will become of me, am I hetero?’ etc) than ‘average’ adolescents. This identity ‘crisis’ almost always resolves within a few years. I believe that it is this group that is now ‘recruited’ by the activists in the field.”
Turning the tide
In his expert report, Dr Roman recounted some of the influences leading to Sweden’s self-correction away from the medicalised gender identity of minors—
The 2018 start-up of GENID,8 in which parents and former patients “were distressed that children had received irreversible pharmacological and surgical treatment and were unsure whether the benefits outweighed the risks.”
A 2019 opinion article “Gender change is a great experiment” in a major Swedish newspaper signed by “perhaps the most famous Swedish child psychiatrist living today,” Professor Christopher Gillberg, together with six colleagues9
The first of the “Trans train” episodes on the flagship investigative journalism program, Mission: Investigate, on Sweden’s public broadcaster10
Media reports of cases of regret and suicide following medicalised gender change
Finland’s 2020 adoption of psychological treatment as the first-line response to gender dysphoria, following a systematic review and under the leadership of psychiatrist and researcher Professor Riittakerttu Kaltiala
A 2020 letter in the journal Pediatrics from child and adolescent psychiatrist Dr Annelou de Vries—a key figure in development of the “Dutch protocol” of puberty blockers followed by cross-sex hormones for minors—warning that the protocol’s benefits reported in 2011 and 2014 studies might not apply to today’s atypical patients with teenage-onset dysphoria
The 2020 High Court victory of British detransitioner Keira Bell over her former clinic, the London-based Tavistock service and, that same year, a systematic review commissioned by England’s National Health Service and reporting a lack of evidence for puberty blockers
The “dramatic reversal” of treatment policy at the Astrid Lindgren’s Children’s Hospital—home to Sweden’s leading gender clinic—where management applied the precautionary principle and ruled there would be no more hormonal treatment of gender dysphoric patients under age 16, with the hospital stating, “These treatments are potentially fraught with extensive and irreversible adverse consequences such as cardiovascular disease, osteoporosis, infertility, increased cancer risk, and thrombosis.” Under this new 2021 policy, patients aged 16-18 would only be treated within ethically controlled clinical trials.
Dr Roman said: “In 2001, a total of two children [under age 18] were diagnosed with gender dysphoria [in Sweden]. In 2021, the number was 440, a 220-fold increase. A total of 12 people under 25 were diagnosed with gender dysphoria in 2001, by 2021 the figure was 1,865.” In 2018, the number of diagnoses of gender dysphoria was 15 times higher than 2008 among girls aged 13-17.
Dr Roman said: “There is a possibility that the majority of patients in the new group [diagnosed with gender dysphoria] have autism or autism-like conditions. In their teens, people with autism have even more concerns about their body and identity than other adolescents.” He cited 2016-18 data showing that 28.9 per cent of girls with gender dysphoria aged 13-17 also had depression (as opposed to only 2.8 per cent of girls of the same age with depression in the general population). The counterpart figure for anxiety disorders was 32.4 per cent of the dysphoria group (but 4.2 per cent in the general population). For autism, the figure for the dysphoria group was 15.2 per cent (1.3 per cent in the general population). For ADHD, the figure for the dysphoria group was 19.4 per cent (4.4 per cent in the general population).
For an exceptional case, Dr Roman gave the example of a patient “who has already begun on these therapies and needed to be given some time to continue until it was appropriate to stop.”
Dr Roman pointed out that the diagnostic category of gender dysphoria, adopted in the Diagnostic and Statistical Manual (DSM-5) in 2013, was largely based on the classic patient profile of males with onset of this distressing condition in early childhood, with diagnosis guided by social roles or behaviour. “In the new group [since roughly 2010], a clear majority are of the female sex, gender dysphoria [starts] at puberty and is based on [self-declared] gender identity. Since the new group differs so much from the group on which DSM-5 is based, many in the Swedish medical community now strongly question the reliability of the diagnosis.” Dr Roman said that under DSM-5, one had to identify the main problem if a patient presented with multiple psychiatric conditions. “In the case of gender dysphoria, an alternative condition is often the main problem. When adequately treating the main problem, other conditions often disappear, which can thus be regarded as secondary to the main problem.”
To desist is to stop identifying as trans or non-binary and re-embrace birth sex before any medical intervention.
On the proposed law for self-declared gender change, Professor Landén also said: “I think the government has confused the individual’s right to personal identity with the right to control the behaviour and thoughts of others. That we have the right to live and express ourselves as we wish, does not mean that we have the right to control how others categorise us. If I—as a man—were to exercise my right to change my legal gender to female, the legal gender will be wrong. With the government’s proposal, I can still force those around me to incorrectly categorise me as a woman when I apply for a job, end up in prison, compete in wrestling or choose a locker room at Friskis & Svettis (a fitness centre). Regulating the behaviour and expression of others in this way is an infringement of human rights, not an enhancement of them.”
Professor Landén expressed these concerns in an article published by the influential newspaper Svenska Dagbladet in 2022. In April this year, Sweden’s parliament passed the contentious law but in a less radical form, enabling those aged 16 and above to change legal gender without a diagnosis of gender dysphoria. Professor Landén’s 2022 remarks are still relevant for countries allowing very young children to change their official sex marker. As for Sweden’s law, The Guardian reported in April 2024: “People will be able to change their legal gender at 16, though those under 18 will need the approval of their parents, a doctor and the National Board of Health and Welfare. Sweden has seen a sharp rise in gender dysphoria cases. This is particularly visible among 13- to 17-year-olds born female, with an increase of 1,500 per cent since 2008, according to the Board of Health and Welfare. While tolerance for gender transition has long been high in the progressive and liberal country, political parties across the board have been torn by internal divisions over the new proposal. A poll published this week suggested almost 60 per cent of Swedes oppose the proposal, while only 22 per cent back it.”
The late Avi Ring, a Norwegian scientist based in Oslo whose child was given cross-sex hormones despite showing signs of mental illness, was co-founder of the parents’ group Gender Identity Challenge (GENID) Scandinavia. Avi died last September. He was a great help to me when I was trying to understand developments in Scandinavia. May his memory be a blessing.
Professor Gillberg’s renowned neuropsychiatry group at Sweden’s Gothenburg University has an international network with activity in the Faroe Islands, Paris, Glasgow, Lisbon, Bergen, Cape Town and Kochi, Japan.
The third episode of the Trans Train investigative series, broadcast in November 2021, reported that 13 children in Stockholm given puberty blockers had “severe side effects, one of whom has a skeleton like an 80-90 year old,” Dr Roman said. “The underreporting of side effects is potentially high.” In the UK, Newsnight, the flagship investigations program of public broadcaster the BBC, applied journalistic scrutiny to the London-based Tavistock clinic. In Australia, the counterpart ABC program, Four Corners, has uncritically promoted medicalisation of gender non-conforming minors.
Great article. Re the ABC, they still have their disgraceful child-grooming video on TikTok, about how great puberty blockers are. All their articles on trans issues support the trans-industrial complex.
So much for investigative journalism.
"In his expert report, dated May 2023, Dr Roman said social transmission of psychiatric syndromes was 'very common,' especially among teenage and young adult females. He cited the examples of anorexia being reinforced among groups of in-patient females, and the practice of sharing images of self-harm on social media."
This is an example of a fact-based scientific finding that trans rights activists and their credulous allies will not tolerate and will seek to discredit at every opportunity. That includes mounting savage attacks on the researchers in order to threaten their careers. They'd say that up is down if it served their cause. They're remarkably effective at getting away with it in the mainstream media.