
Judgment day
Gender dressed up as sex; Alberta's new protection law; trans surgery on German minors; UK adult clinic review; Texas prosecutions; Oz whistleblower asks for votes; AMANDA's award; gagging Dr Haim


GCN in brief
Supreme test
America | Tomorrow, US time, the Supreme Court will hear argument in a test case on whether the American Constitution prevents the state of Tennessee from prohibiting the gender medicalisation of minors. Tennessee is one of 26 Republican-run states to enact restrictions or bans on puberty blockers, cross-sex hormones and surgery for distressed minors who reject their birth sex.
Although there has been much litigation over such laws at lower levels of the court system, Tennessee’s is the case that the Biden administration—an aggressive promoter of “gender-affirming care”—decided to challenge before the highest tribunal in the nation, the Supreme Court, where legal conservatives are a majority on the nine-strong bench of judges. The Tennessee law, known as SB1, was ruled valid by the US Court of Appeals for the 6th Circuit last year.
The US government’s argument is that SB1 is invalid because it discriminates on the basis of sex and breaches the equal protection clause of the Constitution’s fourteenth amendment. The government’s petition says: “SB1 classifies based on sex, through and through… [It] bans puberty blockers and hormone therapy if—and only if—those treatments are provided ‘for the purpose’ of ‘[e]nabling’ an adolescent to identify with a gender ‘inconsistent with the minor’s sex’ or treating distress ‘from a discordance between the minor’s sex’ and gender identity.”
Puberty blockers would still be available in the state for the purpose of treating minors with precocious puberty. It is the sex of the patient, according to the US government, that decides whether or not the medicine is for a prohibited purpose. “SB1 restricts care only for transgender individuals who seek to induce physiological effects inconsistent with their sex assigned at birth.”
In response, Tennessee’s Attorney-General Jonathan Skrmetti insists that SB1 “does not classify based on sex. At most, it draws lines based on age and the nature of the medical intervention. Certain medical interventions may not be administered to minors for certain purposes, but boys and girls are treated equally.” That is, neither boys nor girls may be given medical treatment to transition their gender.
Mr Skrmetti also says the law does not “treat similarly situated individuals differently based on their sex. An adolescent boy might be given testosterone to correct a deficiency and restore the biological baseline. But that boy suffering from a disorder (testosterone deficiency) is in no relevant sense similarly situated to an adolescent girl suffering from gender dysphoria who is administered testosterone to induce different physical traits than would otherwise develop.”1
On the wider context, Mr Skrmetti says: “States across the country are facing a surge of minors receiving gender-dysphoria diagnoses and being administered unproven and risky medical interventions with potentially irreversible effects on their health and fertility. The question here is whether the Constitution prohibits Tennessee from acting to protect minors who may not fully grasp the lifelong implications of these interventions.”
There are other cases involving paediatric gender medicine which did not go up to the Supreme Court, but are already affording many mainstream people a warts-and-all glimpse inside the gender medicine machine. A challenge to Alabama’s law banning these interventions—a law similar to Tennessee’s—has spilled into the public domain a vast number of internal documents damaging to trust in gender-affirming care.
As journalist Lisa Selin Davis explains in the Boston Globe, “Over and over in the evidence uncovered by these lawsuits, we see the government organizations, medical associations, advocacy groups, and clinicians that insist on the safety and efficacy of youth gender medicine admitting, and hiding, the opposite.
“WPATH [the US-based World Professional Association for Transgender Health], AAP [the American Academy of Pediatrics], and [the US Department of Health and Human Services] twisted and concealed evidence, lied about research, protected and enriched themselves and their members, and politicized science. They indemnified practitioners instead of protecting patients. They are unfit to manage the care of increasing numbers of gender dysphoric young people in America.”
For an eye-opening introduction to the various players in tomorrow’s Supreme Court drama, courtesy of lawyer Glenna Goldis, go here. As for WPATH, it is seeking a new executive director whose duties include expanding the organisation’s “global impact as a leader in transgender health.” Competitive medical benefits are part of the package.
Video: What to expect when the Supreme Court hears the case US v Skrmetti
Save the future
Canada | The province of Alberta has passed legislation to prohibit trans surgery for minors and stop new prescriptions of puberty blockers or cross-sex hormones for gender-distressed children under age 16, as foreshadowed in February by United Conservative Party Premier Danielle Smith. “These policies are designed and intended to help preserve the choices children have before they make serious decisions about their bodies or the ability to have children of their own one day or undergo potentially permanent procedures where the benefits and risks are not yet fully understood,” Premier Smith said on October 31. The legislation passed its third reading in the legislative assembly on December 3.
The statute is known as Bill 26: Health Statutes Amendment Act 2024 (No. 2). In her second reading speech on November 5, Ms Smith noted the shift towards caution in the UK and Sweden. She quoted endocrinologist Dr Roy Eappen, a senior fellow at US watchdog group Do No Harm, welcoming Alberta’s policy as providing “essential guardrails” and protecting “young individuals during a formative period in their lives, ensuring their choices align with their long-term wellbeing.”
The candidate
Australia | Whistleblower child and adolescent psychiatrist Dr Jillian Spencer has announced she would like to run for president-elect of the Royal Australian and New Zealand College of Psychiatrists. Nominations close on December 17. Dr Spencer was suspended in 2023 by a public children’s hospital in the state of Queensland after she questioned the safety of the gender-affirming treatment model. On Twitter/X last Saturday, she said the college’s response to the issue of harm to children from gender medicine was “shockingly inadequate.” In her opinion, the college had “permitted advocacy and ideology to replace scientific rigour.”
“[T]o retain the trust and respect of the community, the college needs to urgently call for an end to the gender-affirming model of care for children and adolescents with gender distress. This is crucial, because it is the failure of the medical colleges to speak out that has allowed Australian politicians to also avoid their responsibility.”
With a new centre-right government in Queensland, veteran journalist Des Houghton wrote in Saturday’s Courier Mail newspaper that Dr Spencer was owed reinstatement and an apology. Citing England’s Cass report, Mr Houghton suggested it was time for Liberal National Party Premier David Crisafulli to act by imposing a ban on puberty blockers.
Still immature brains
United Kingdom | A review of adult gender clinics within the National Health Service (NHS) England will examine operating procedures, how the service model meets patient needs, challenges in service delivery, and any action to improve effectiveness and safety. Terms of reference issued on November 14 also state that the review, to be led by Dr David Levy, “will escalate current safety concerns where required to protect patients at the earliest opportunity to allow action to be taken to address issues.” The majority of those on waiting lists for NHS adult clinics are reportedly under age 25 and female.
Meanwhile, a judicial review challenge to the licensing of a private clinic, GenderPlus, has been allowed to go ahead. GenderPlus has been registered by the Care Quality Commission to give hormonal treatment to 16- and 17-year-old patients. The judicial review in the High Court is being brought by an anonymous parent and psychotherapist Sue Evans, who was an early whistleblower at the Tavistock clinic. The crowd-funding campaign for the case has less than three weeks to run.
Left behind
International | A guest editorial in praise of puberty blockers, published by the American Journal of Bioethics, has been challenged by the philosophers Dr Moti Gorin of Colorado State University and Dr Jilles Smids of the Erasmus University Medical Centre. In a letter, they took issue with various claims, including the suggestion that blockers merely “pause” puberty and are reversible. “Since the peers of the patient receiving puberty blockers do not have their puberty blocked and since puberty involves not only physical but related and very significant psychosocial development, speaking of ‘pausing’ puberty is misleading,” Drs Gorin and Smids wrote.
¡Enhorabuena!
Spain | The parents’ group AMANDA has been honoured with the Ana de Paz Foundation Award for its “advocacy of prudence and good professional practice to avoid irreversible outcomes.” AMANDA is the Spanish acronym for Group of Mothers of Adolescents and Children with Rapid-onset Gender Dysphoria. Ana de Paz Nieto worked for 20 years as a teacher in the dedicated classroom at the La Paz Hospital in Madrid, educating children with cancer and other serious illnesses.
Conflicted
America | Tina Ansari, the prosecutor leading the US Department of Justice case against whistleblower Dr Eithan Haim, has been withdrawn from the case after Dr Haim’s legal team raised “serious ethical questions” about her conflicts of interest. Ms Ansari was said to have “close family members have substantial financial and political ties” to Texas Children’s Hospital and Baylor College of Medicine. Dr Haim, a surgeon, is accused of unauthorised access to patient records of the children’s hospital during his residency at Baylor college. He had passed de-identified records to a journalist to prove that the children’s hospital, contrary to its public assurances, had not ceased to practice gender medicalisation on minors.
In the Haim case last month, the US Department of Justice sought a gag order, citing fear of “online bullying” of its prosecutors resulting from Twitter/X commentary by Dr Haim, who faces a ten-year prison sentence if found guilty and has had to crowd-fund his defence. Dr Haim tweeted: “[The department’s prosecutors] zealously deploy the threat or the outright use of state-sanctioned violence against those who challenge their political ideology yet cast themselves as the victim when regular citizens stand up, take notice, and utilize their first amendment right to criticize their tyrannical behavior.”
Iatrogenic medicine
International | There may be a link between cross-sex hormone treatment and testicular cancer, according to a new study published in the Archives of Pathology & Laboratory Medicine based on analysis of surgically removed testicles. The incidence rate of neoplasms in 458 specimens from “gender-affirming orchiectomies” over a 5.5-year span was 27 times higher than the rate for the general population. “The higher incidence rate of testicular cancer among transgender females [males] in our series may be due in part to maturation arrest from pretreatment with hormones or blockers, a known risk factor for testicular cancer,” the study authors wrote.
Meanwhile, in a recent comment article in the Annals of Pharmacotherapy, endocrinologist Dr Michael K Laidlaw and pharmacist Dr Sarah Jorgensen suggested that the emotional distress and psychiatric symptoms linked to high-dose cross-sex hormones might be a factor in the elevated suicide risk among trans-identifying people. They cited the suicides of two young people within two years of starting cross-sex hormones in a 2023 study by Chen et al. This represented a suicide rate of 317 per 100,000 per year, compared with a rate of 13 from the world’s largest paediatric gender service, the London-based Tavistock clinic. Drs Laidlaw and Jorgensen were commenting on a study of adverse drug reactions to trans hormonal treatment reported to the US Food and Drug Administration.
Doctors in the dock
America | Texas Attorney-General Ken Paxton has sued two more doctors for alleged breaches of consumer protection provisions and a 2023 law prohibiting gender medicalisation of minors. The first doctor, sued on October 17, was Dr May C Lau. Now, Dr Hector M Granados of El Paso—described in a court document as a “radical gender activist”—stands accused of using the false diagnosis of precocious puberty to disguise the fact he was giving children as young as age 12 hormone suppression drugs to interrupt naturally timed puberty and thereby affirm their non-biological “gender identity.”
Dr Granados allegedly misled pharmacies, insurance providers, and/or the patients by falsifying patient medical records, prescriptions, and billing records. He is also said to have unlawfully given testosterone to 14 transgender-identified females, the youngest aged 14, under the false diagnosis of “endocrine disorder, unspecified.” These girls, it is alleged, were falsely listed in medical records as male.
The third medical defendant is Dr M Brett Cooper of Dallas. He allegedly prescribed testosterone as a cross-sex hormone for 15 girls, the youngest aged 16, sometimes falsely recording these patients as male in medical records. Dr Cooper is also accused of falsely diagnosing patients with precocious puberty and endocrine disorder and using these conditions to bill insurers.
The court filing against him cites his Twitter/X posts—with the handle TeenDocMBC—as evidence that “he infuses his medical practice with radical gender activism and exercises poor judgment…” For example, in 2020, Dr Cooper allegedly tweeted about a 17-year-old female patient that, “She may be the second patient I urge to get emancipated. One of my [female] trans guys I actually encouraged to move out of his mom’s house at 17 and just get declared emancipated.” His Twitter/X profile describes him as a “medical educator.”
Scalpel cuts through law
Germany | The number of genital surgeries—so-called “sex-change operations”—in Germany has exploded in the age group of 18-25 years, according to doctoral student of economics Paul Steger, whose Substack newsletter scrutinises gender issues. The increase, he reports, is 12,312 per cent, from eight operations in 2005 to more than 985 in 2023, representing a total of 6,404 surgeries for that age group over almost two decades.
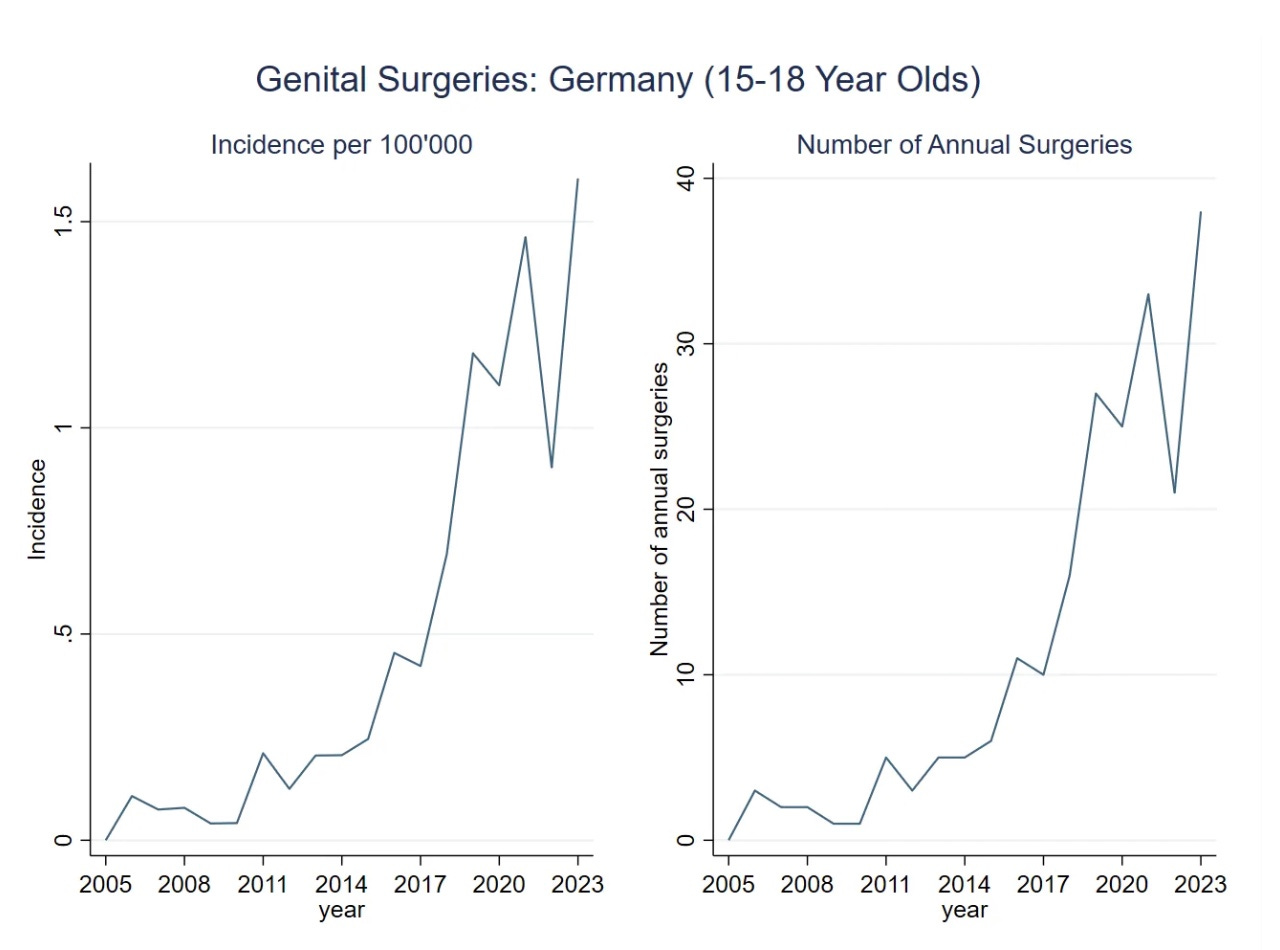
As for genital surgeries involving minors, Steger notes, German law prohibits medical interventions resulting in the sterilisation of minors, unless these are necessary to save a patient’s life. The data tells a different story. “While the absolute numbers [of genital surgeries for patients aged 15-18] remain low, their explosive growth suggests that more are yet to come.” Steger cited the principle of “trans exceptionalism” to explain this medical defiance of the law, while “policymakers and journalists remain largely oblivious to the phenomenon.”
Chart: Gender surgery on the rise among minors
Fresh data
Meanwhile, cases of “gender identity disorder” among patients aged 5-24 rose eightfold in Germany from 2013 to 2022, according to an analysis of insurance data. “The increase was particularly pronounced among biologically female adolescents aged 15 to 19,” the magazine Spektrum.de reported in October.
“Three quarters of young people with gender dysphoria were found to have another psychiatric diagnosis, most commonly depression, borderline disorder, attention deficit hyperactivity disorder or post-traumatic stress disorder. The gender incongruence turns out to be rather unstable over time: after five years, more than half of those affected no longer had gender dysphoria. However, the data did not allow the causes of the trend to be identified.” David Allison of Transteens Sorge berechtigt, a lobby group critical of gender medicalisation, told GCN this was “the first and therefore the most important statistical data we have ever received for Germany.”
The country’s self-ID gender law took effect on November 1. The government has “the under-the-radar aim of promoting gender medicine,” Mr Allison said in an article published by Genspect. “Politicians argue that the self-ID law is unrelated to medical interventions. The evidence from the Tavistock in London and the conclusions of the Cass review—in particular the recognition that social transition is not a neutral act and that puberty blockers set off a cascade of increasing medicalisation—is ignored.”
In the German-language Corrigenda magazine, Laila Mirzo gave an account of how she almost lost her daughter to transgender medicalisation and “an existential crisis in which the state also aggressively interfered.” The child declared a trans identity at age 11 and Mirzo, who edits a German Jewish newspaper, was caught “completely off guard” by the insistence of doctors that invasive medical treatment was a matter of urgency.
“I was even accused of ‘endangering the welfare of the child’ because I mentioned my daughter by her so-called ‘dead name’, her discarded birth name, in an email to the youth welfare office, instead of using the gender-neutral name she had chosen… The situation became more and more absurd and almost Kafkaesque. I had no chance against this superior power, which in the event of non-cooperation even threatened to withdraw custody from me.”
The way Mirzo saw it, “this hype about ‘transsexuality’ is a kind of youth movement. In my daughter’s school class alone, about a quarter of the children were officially ‘transsexual’.” Three years later, after a summer holiday away from her clique and a change of school, the girl took “the opportunity to reinvent herself, or rather, to find herself again.”
Testicular trouble
Australia | A substantial share of taxpayer-funded testosterone appears to be used by trans-identified females to masculinise their bodies, according to a study published in the Medical Journal of Australia. The majority of people aged 40 and younger receiving subsidised testosterone from July 2021 to June 2022 appeared in the data with a current or past female marker, suggesting this was cross-sex hormone treatment. The authors note there is no indication for this use under the publicly funded Pharmaceutical Benefits Scheme (PBS). In order to access PBS-funded testosterone, gender clinicians use the indication for the male condition “androgen deficiency due to an established testicular disorder.”
No consensus
America | Last month, country circuit court Judge R Craig Carter threw out a challenge to Missouri’s law restricting paediatric gender medicine. “This court finds an almost total lack of consensus as to the medical ethics of adolescent gender dysphoria treatment,” Judge Carter said. “The evidence at trial showed severe disagreement as to whether adolescent gender dysphoria drug and surgical treatment was ethical at all, and if so, what amount of treatment was ethically allowable. States do have abiding interest in protecting the integrity and ethics of the medical profession.” Missouri enacted its law after whistleblower Jamie Reed revealed disturbing practices at the Washington University youth gender clinic in St Louis.
In The Economist magazine’s preview of the US v Skrmetti case, healthcare researcher Zhenya Abbruzzese of the Society for Evidence-based Gender Medicine was quoted as saying that the parties promoting teen gender transition, such as the Biden administration, were “trying to appropriate the [constitutional] protections of sex, and substituting it with gender identity.”
The Royal Children's Hospital Gender Service website: it “aims to improve the physical and mental health outcomes of children and adolescents who are trans or gender diverse”. While the outcome following transition is said to be rosy for the ‘newly-gendered’ children it is reasonable to ask how will it be for them in the long term thirty, forty or fifty years?
There are few studies that investigate the long-term outcome (40 or 50 years) following ‘transition’. Is there a time when the honeymoon is over?
I reference two peer reviewed studies that looked at thisl:
• ‘Long-Term Follow-Up of Transsexual Persons Undergoing Sex Reassignment Surgery: Cohort Study in Sweden (1973-2023)’
All 324 sex-reassigned persons (191 male-to-females, 133 female-to-males) in Sweden over the period 1973–2003 were studied. Random population controls (10∶1) were matched by birth year and birth sex or reassigned (final) sex, respectively.
Conclusions: Persons with transsexualism, after sex reassignment, have considerably higher risks for mortality, suicidal behaviour, and psychiatric morbidity than the general population..
• ‘Trends in suicide death risk in transgender people: results from the Amsterdam Cohort of Gender Dysphoria study (1972–2017)’
To study the overfall suicide death rate, the incidence over time, and the stage of transition where suicide death were observed in transgender people
A chart study, including all 8263 referrals to our clinic since 1972.
Conclusions: The suicide risk in transgender people is higher than in the general population and seems to occur during every stage of transitioning.
These two studies suggest that “the aim to improve the physical and mental health outcomes of children and adolescents who are trans or gender diverse” may not be met through ‘gender-reassignment’.
Perhaps something a little more conservative would be appropriate?
I enjoyed the philosophy letter. I had it in my notes over the last 20 years…
1. There is no valid concept of temporary pause in progress to adult maturity during puberty, only partial deletion.
2. A child which has pubertal maturation disrupted cannot make up for lost time, that is a physical impossibility.
3. Like a trip of 101 days, if you are blocked for 100 days, resuming at normal speed you cannot make up the missing 100 days in one day. It’s physically impossible.
4. The leadership, including past presidents of WPATH, have spoken to this fact in public, on record.
5. Among other uses in adults, endocrine disruptors used to disrupt puberty in children create sterilization in men as treatment for prostate cancer. They are sterilizing agents.
6. Puberty disruptors are time-release sterilization, the earlier they begin and the longer they persist the more complete the sterilization in all children, boys and girls alike.
7. Sexual maturity occurs simultaneously with a variety of complex processes including but not only pre-adult phase synaptic pruning and release of Human Growth Hormone driving bone maturation and physical growth.
8. At least all three must operate in synchrony to arrive at complete adulthood even beyond sexual function.
9. There is no “maturity accelerator” to compensate for disruption and desynchronization among the different drivers of adult maturation.
10. In some children, sexual maturation begins early, out of synch with physical growth, mental, and skeletal maturation,
11. In such children sexual maturation is disrupted until it can be brought in synchronization with natural skeletal, mental, and physical growth and maturation.
12. Use in children after skeletal, mental, and physical growth and maturation begins, acts precisely to desynchronize natural critical synergistic processes the opposite purpose it was intended for in children.
13. Damage is far more extensive than sterilization.
14. The die is cast at conception for being male or female, by genetic material from the sperm.
15. Human males go through three puberties: the first a few weeks after conception, the second immediately after birth. The first two prepare the body for the third, which occurs slowly in the decade preceding adulthood. The third completes the process.
16. Final puberty can only be disrupted, never extended or accelerated or resynchronized with other maturation processes.
17. Due to disruption of intellectual maturation which requires natural hormonal environments, all children remain partially or completely unable to attain intellectual ability as adults.
18. Due to disruption of natural hormonal environments required for bone growth, all children have partially or completely insufficient bone density to sustain them for a lifetime.
19. Sex “Dysphoria” during puberty is primarily a result of gay or lesbian self-realization along with bullying, self-doubt, anxiety and fear.
20. Unhappiness at the beginning of puberty is not unusual, goes away the more complete puberty becomes.
21. Sufficient disruption of maturation can make the dysphoria permanent.
22. Children and adults who have been misled into believing that disrupting puberty can alleviate unhappiness due to emergent homosexuality, can be convinced that even more hormonal disruption will complete the process.
23. Children and adults can be likewise misled that the solidified dysphoria can be remedied by even more extreme hormonal disruption.
24. The entire exercise is a form of child sexual abuse, similar to barbaric female and male genital mutilation and sterilization.