
It's the biggest scandal of my time in medicine
A distinguished Australian physician reflects on the troubling trend of gender medicalisation for vulnerable minors

Gary Geelhoed
It must be confusing for mainstream people trying to make sense of the increasing coverage and complexity of the transgender issue in Australian society. They are well aware of past inequalities for women, the gay community and various racial groups both in the legal sense and in terms of their treatment in wider society. Given that these groups now have full recognition under the law and more generally in society, many people are now also sympathetic to an apparently new minority, trans people, facing what could be perceived to be similar challenges.
The LGBTQ+ alphabet groups, while often lumped together, in reality have little in common and increasingly the trans group is at odds with the lesbian group over the definition of the term “woman”. Also, it is becoming increasingly clear that many young, confused people who are same-sex attracted are being encouraged into the trans group.
Most people believe adults should be allowed to identify as they like, dress as they like and love who they like, as long as no one else is harmed. The issues around the emergence of transgender folk, however, are more complex when it comes to children and adolescents.
The characteristics of previously discriminated-against groups—women, ethnic minorities and the same-sex attracted—remained fixed as society changed to a more sympathetic view. But a core belief of trans individuals is that their gender is what each individual identifies it to be, not what society might deem it to be. Those other once-marginalised groups asked to be accepted as they are. Trans individuals ask that society recognise them as the sex or gender opposite to that with which they were born.
This may go beyond superficial aspects such as dress, hair and makeup to permanent medical treatments and procedures such as puberty blockers and cross-sex hormones, as well as surgery to remove breasts or to create approximations of a vagina or penis. Many people are sympathetic to adults who feel driven to go down this path and to make such serious decisions.
Historically, there has always been a very small percentage of the population, mainly boys, who at a very early age identify as the opposite sex. The majority of these children in time would go on to re-identify as their original sex with many growing up as same-sex attracted. Another well-recognised group were middle-aged men who chose to live as women but generally did not regard themselves as actual women.
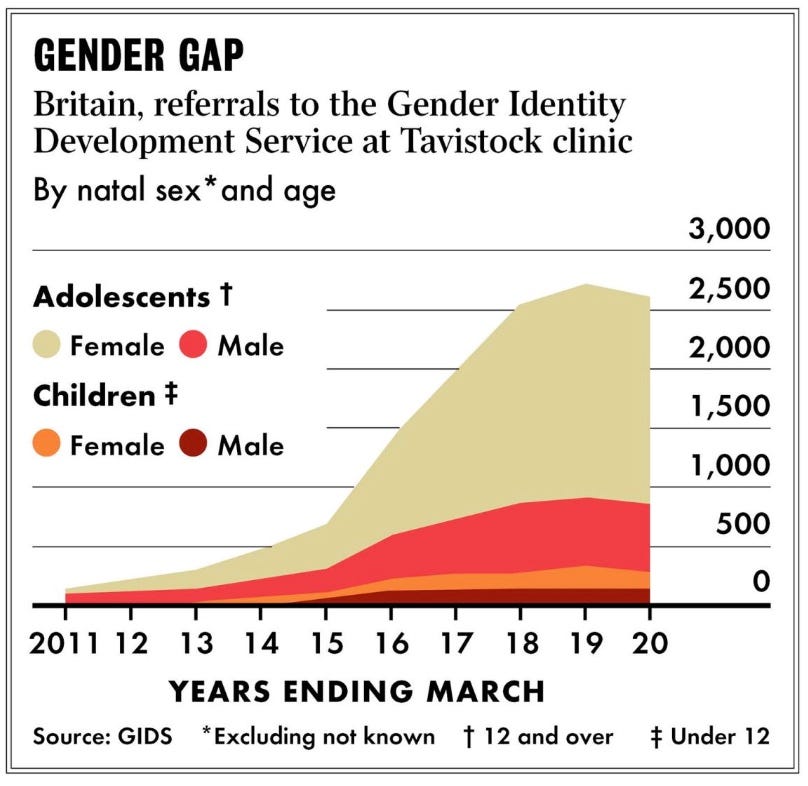
What has changed, largely across the Anglosphere, is that the number of children and adolescents who now wish to transition to the opposite sex has grown exponentially, with the majority now being female at birth. Often, they have shown no inkling prior to “coming out” that they were transgender, hence the term ROGD (Rapid-Onset Gender Dysphoria). A significant number are same-sex attracted and many are on the autistic spectrum.
Chart: Referrals at the London-based Tavistock clinic dramatically illustrate the international shift in patient profile from a small number of male children to very many female adolescents
Child safeguarding
While many people support or at least try to understand adults who wish to transition, they are troubled that increasingly younger individuals are being guided down this path. To be very clear, the current discussion on the best approach to children and young adolescents who identify as trans should not be clouded by reference to social inequalities in the past for the LGB community or the decision of an adult to transition to the opposite sex. The concern is for the increasing numbers of children and adolescents taking this largely one-way, lifelong path of medicalisation.
While not allowed to drive, vote or even have tattoos, young people are allowed in increasing numbers to decide they are in the “wrong body”. In many jurisdictions, responsible adults, including parents and health professionals, are expected to “affirm” this choice. Resistance or even a more nuanced “wait and see” approach—while addressing other possible mental health issues—is being labelled “transphobic”. In some jurisdictions, the “wait and see” approach is in effect prohibited under law.
It seems clear that confused and troubled young people are attracted to the idea that changing gender will improve their lives and, in many cases, the positive affirmation they receive—and in some cases, testosterone treatment—may achieve this in the short term. The good intentions of gender clinic staff are not in question.
Usually, this sudden realisation in young adolescents that they are in the “wrong body” is the first inkling that parents have. More worrying is the small number of parents who appear to be driving the process from a child’s young age, a practice that once would have been labelled as Munchausen by Proxy.
Affirmation for parents may mean agreeing with their teenage daughter’s decision to block her pubertal development, take lifelong medications and surgery rendering her infertile and with impaired sexual function.
What is increasingly clear is that this great increase in numbers over the last ten years coincides with the advent of social media. Repeatedly, young people attest to both discovering the concept of transgenderism online and being directly influenced to explore further, often in social clusters.
Video: Physician and researcher Dr Lisa Littman, who coined the term ROGD, outlines early results from a significant new study of today’s markedly different caseload of gender-distressed youth. This was a key presentation at Genspect’s 2025 conference in Albuquerque, New Mexico.
Spotlight on medicos
Troubled young people struggling with the transition to adulthood are being encouraged and celebrated for identifying as the opposite sex. Once this might have been a time of confusion from which the majority would emerge as intact young women coming to terms with their sexuality and perhaps autism and depression. Increasingly, however, these young people enter adulthood on lifelong medication, some with radically surgically altered bodies and sterility. All this with very little evidence to attest to the long-term positive outcomes promised and increasing evidence of the problems associated with long-term medications and surgery.
Because of this, a very bright spotlight should be trained on the medical profession which controls and permits the administration of puberty blockers, cross-sex hormones and surgeries. The history of medicine is littered with many dark dead-ends which at the time were trumpeted as great advances. Among these were removal of children’s tonsils unnecessarily, extraction of all healthy teeth to prevent caries, removal of healthy large bowels (colons) assumed to be toxic, and the equivalent of waving a knitting needle in frontal lobes, lobectomy, to treat various mental disorders.
Modern medicine strives to be evidence-based but evidence for the diagnosis and treatment of ROGD is lacking. For instance, the oft-quoted “better to have a live son than a dead daughter” deployed to influence parents is not supported by any meaningful study. While there may be adults who have transitioned in the past after careful and long consideration who now lead happy lives, there are no long-term studies showing that on balance this is the usual experience. The evidence for this new cohort of ROGD adolescents is virtually non-existent, given their short history.
We do, however, know that the physiological and anatomical changes of drugs and surgery are lifelong. The standard in the past was to only go down the trans path, recognising its rarity, after other approaches and explanations had been worked through. The more recent phenomenon of young girls being affirmed and placed on the trans treadmill after only a short period, with other factors and explanations largely ignored, is very different.
The experience at the London-based Tavistock Gender Identity Development Service (GIDS), which operated for decades in the UK, is instructional.
An independent report by consultant paediatrician Dr Hilary Cass, a former president of the Royal College of Paediatrics and Child Health, concluded that GIDS was “not safe” and suggested a need for a “fundamentally different” service. As such, GIDS closed in 2024 and was replaced by regional hubs with a more holistic approach allowing for all issues in young peoples’ lives to be examined when presenting with confused identities.
The risks of medical harm and regret are exemplified by the story of the Tavistock GIDS detransitioner Keira Bell, a troubled teenager who at the age of 16 was prescribed puberty blockers followed by testosterone a year later; at 20, she had a double mastectomy. “But the further my transition went, the more I realised that I wasn’t a man, and never would be,” she recalls. “We are told these days that when someone presents with gender dysphoria, this reflects a person’s ‘real’ or ‘true’ self, that the desire to change genders is set. But this was not the case for me. As I matured, I recognised that gender dysphoria was a symptom of my overall misery, not its cause.”
In the UK, following the Cass review, bipartisan policy has ended the routine use of puberty blockers for gender-distressed minors outside a clinical trial scheduled to start this month. Other European nations, New Zealand, half of America’s states and Queensland have paused, banned or restricted the gender medicalisation of minors. It is time that Australia as a whole follows suit. In my own state of Western Australia, the release of the model of care for the gender clinic at the Perth Children’s Hospital gives rise to the same kinds of concerns occasioned by the ideological “gender-affirming” treatment model elsewhere in the world.
The tide of opinion is turning as more people become aware of this very specific problem of young adolescents being affirmed and subjected to lifelong medical and surgical consequences. They realise this is very different to the now largely dissipated wider discrimination against the LGB community.
I am now at the end of a long career in medicine. I trained as a general paediatrician, ran a tertiary paediatric emergency department for 22 years, was a federal councillor of the Australian Medical Association and an AMA WA President. I was Chief Medical Officer and Assistant Director General for the WA Department of Health for five years.
In my opinion, the current treatment of gender-confused minors is the biggest medical scandal of my time in medicine. While I respect the rights of adults to identify and live how they wish, I call on the profession to objectively look at the evidence—or rather, the lack of it—in this complex area of paediatrics. And I urge the profession to advocate for the banning of puberty blockers, cross-sex hormones and surgery for these vulnerable minors.
Professor Gary Geelhoed is a retired paediatrician and researcher who served as Chief Medical Officer of WA and directed the emergency department of the Princess Margaret Hospital for Children, which was succeeded by the Perth Children’s Hospital, home to a gender clinic. His comments on that clinic’s model of care, and the gender-affirming treatment approach generally, are reported in The Weekend Australian newspaper today.
Bernard Lane can we nominate you for Australian Of The Year ? To do so we need your permission/ knowledge/age group/ an email, which I would like to share on X and FB? https://australianoftheyear.awardsplatform.com/entry-form/entrant/kYnMALaL/edit?tabSlug=gjeXqKYN
If only more people had the courage to say what they really think, like this good doctor.