
Blind to autism
The Cass review picks up an Australian gender clinic not screening for autism


The gist
England’s Cass review has revealed that the fast-growing gender clinic of an Australian children’s hospital does not screen new patients for autism.
In an international survey commissioned by the British paediatrician Dr Hilary Cass, one of five unnamed Australian clinics reported that it does not screen for autism because it claims such screening is “not accurate in [the] trans population.”
Clues in survey responses suggest this is the gender clinic at the Queensland Children’s Hospital in Brisbane, which also has the quickest fast-track to puberty blockers for children as young as age 8-9.
Patient numbers there reportedly rose from 190 in 2017 to 922 in 2022. In 2019, the Queensland clinic had more than 200 minors on puberty blockers1. Also in 2019, a concerned member of the public asked the clinic how many girls with autism were on blockers and was told no such data was kept.
Two other Australian gender clinics in the Cass-commissioned survey—identifiable as those at the Royal Children’s Hospital Melbourne (RCH) and the Perth Children’s Hospital [PCH]—use the Social Responsiveness Scale (SRS) to screen for autism traits.
The results of this screening test do not amount to a formal diagnosis but can identify children for referral to an autism specialist for diagnosis. A 2019 study stated2 that the PCH gender clinic “does not have capacity and resources to formally diagnose [autism].”
Youth gender clinics in Denmark, Finland and the Netherlands use the Autism Diagnostic Observation Schedule for screening, according to the Cass survey.
The over-representation of minors with (sometimes undiagnosed) autism in gender clinic caseloads internationally is a key concern in the debate3. One theory is that gender confusion may be a product of children with autism being immature and desperate to fit in, having rigid and concrete styles of thinking, and obsessional interests.
RCH in Melbourne has reported that 16 per cent of a patient sample had autism4. The prevalence of autism in the general population of Australian children is thought to be less than three per cent.
A psychologist whose daughter attended the Queensland gender clinic told GCN that in her experience “the psychological assessment was not thorough, and no history of trauma5 was taken.”
“If they are not digging deeper to carefully screen for trauma and neurodivergence and treating these issues, then they are applying very poor science,” she said.
Clinical psychologist Dr Vanessa Spiller pointed out that screening for autism was recommended by the first clinical guideline for co-occurring autism spectrum disorder (ASD) and gender dysphoria in adolescents.
“Diagnosing [gender dysphoria] can be complex in adolescents with ASD due to ASD-related weaknesses in communication, self-awareness, and executive function6,” the 2016 guideline by Strang et al says.
Dr Spiller told GCN that in her opinion, it would be negligent for a gender clinic not to take into account the effect of autism and its impairments on a minor’s capacity to make decisions and give informed consent to medical treatment.
Last month’s Cass report says England’s new regional services to replace the London-based Tavistock gender clinic should include autism specialists in their multidisciplinary teams, and standard assessment of new referrals should screen for autism and other neurodevelopmental conditions.
A Cass-commissioned evaluation of international treatment guidelines includes the 2018 “Australian standards of care” document issued by RCH in Melbourne and used across Australia’s youth gender clinics.
The Cass researchers note that the RCH guideline is among the majority of guidelines in which the recommended domains for assessment do not include neurodiversity or autism7.
Video: US whistleblower Tamara Pietzke objected to seriously disturbed children, some with autism, being “affirmed” and given hormonal interventions
The detail
Australia’s Health Minister Mark Butler has played down the relevance of the Cass report, saying that “the clinical pathways are different in the UK from Australia.”
Last month, Western Australia’s Liberal leader Libby Mettam, who is in opposition, cited the influence of the Cass report when announcing a policy to prohibit puberty blockers, cross-sex hormones and trans surgery under the age of 16, pending a comprehensive review.
“The need for urgent action is compounded by the rapidly growing number of children being diagnosed and treated for gender dysphoria in [Western Australia],” Ms Mettam said. “Our review will also inquire into why we are seeing this rise in diagnosis.
“There are currently more than 100 children and adolescents being treated at Perth Children’s Hospital with either puberty blockers or cross-sex hormones, with the youngest aged 11.
“When experts are telling us the potential permanent side effects of these treatments can include infertility, sexual dysfunction, obesity, heart and liver disease, blood clots and atrophy of the genitals, we need to investigate.”
In line with England’s Cass report, Scotland and Wales have announced restrictions on puberty blockers.
In Canada, Alberta’s premier Danielle Smith said the Cass report vindicated her province’s plans to prohibit blockers and cross-sex hormones for minors aged 15 and under. She said she had spoken to Dr Cass to better understand her report.
“If we want to take a science-based approach, we’ve got to use the best information available,” Ms Smith told the National Post.
In the US, South Carolina has moved closer to becoming the 25th state to restrict medicalised gender change for minors.
Behind the mask
The Cass report cites research suggesting that those who identify as transgender or non-binary are three to six times more likely to be autistic than the general population.
“These findings are echoed by clinicians who report seeing teenage girls who have good cognitive ability and are articulate, but are struggling with gender identity, suicidal ideation and self-harm,” the report says.
“In some of these young people the common denominator is undiagnosed autism, which is often missed in adolescent girls.
“Despite often being highly articulate, intelligent and skilled in many areas, autistic young people have difficulties with social communication and peer relationships, which may make it difficult for them to feel accepted and ‘fit in’.”
In her book on the scandal at England’s Tavistock gender clinic, journalist Hannah Barnes recounts how some staff were “stunned” by the clinic’s poor data collection when this was revealed in court proceedings brought by detransitioner Keira Bell.
“[The clinic] could not even tell the High Court how many of the young people put on blockers were autistic,” Ms Barnes writes in Time to Think.
“Some staff feared that they could perhaps be unnecessarily medicating autistic children. Less than two per cent of children in the UK are thought to have an autism spectrum disorder. Yet, according to [the Tavistock], ‘around 35 per cent of referred young people present with moderate to severe autistic traits’.”
In 2020, the regulatory Care Quality Commission (CQC) inspected the clinic.
Ms Barnes writes: “In a sample of records of young people referred for puberty blockers, the CQC found that more than half referred to autism spectrum disorder or attention deficit hyperactivity disorder. Yet, the regulator noted, [the Tavistock] generally did not record how many patients had a diagnosis or a suspected diagnosis of autism spectrum disorder. ‘Records did not demonstrate consideration of the relationship between autism spectrum disorder and gender dysphoria’ or that the needs of autistic patients had been ‘fully investigated’.”
“It wasn’t that anyone thought that it was not possible to be both autistic and trans, but clinicians openly questioned whether the over-representation of autistic young people [at the Tavistock] warranted pause for thought and a change in practice.”
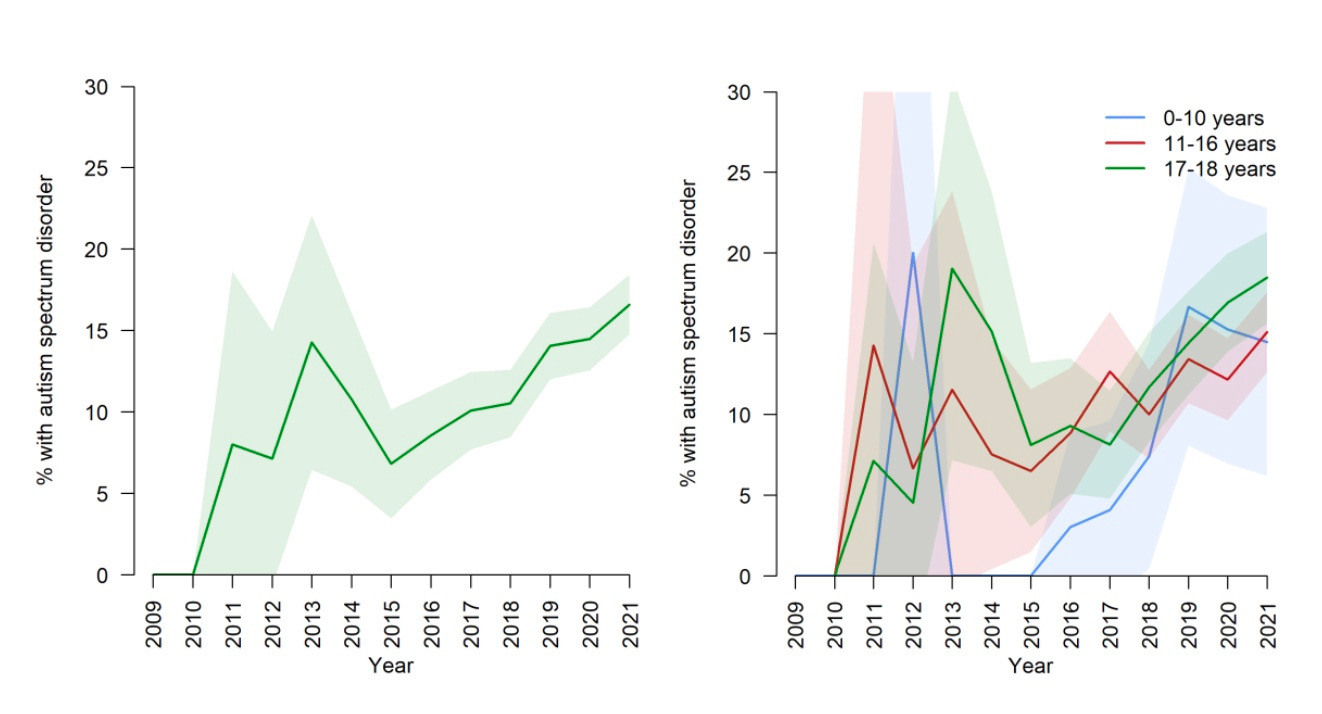
Charts: Co-occurrence of gender dysphoria and autism spectrum disorder, overall and by age group
Under the waterline
The psychologist whose daughter was seen by the Queensland gender clinic told GCN that in her opinion the approach to assessment there “put the cart before the horse.”
“Gender dysphoria is similar to other psychological conditions disproportionately affecting teen girls and young women, in that we see obsessional rumination related to identity, appearance and the changing body,” she said.
“But it’s the tip of the iceberg. Underneath the presenting issues, we almost always find neurodivergence and/or trauma and/or anxiety disorders, and shame. [The Queensland gender clinicians] are, in my opinion, missing everything under the waterline.”
The psychologist, whose daughter in time re-embraced her birth sex, was sceptical about the clinic’s stated reason for not doing autism screening.
“What is about this so-called ‘adolescent trans population’ that means standard [autism] assessments used the world over with young people are not suitable for these young folk?”
Clinical psychologist Dr Spiller said the Queensland clinic might be correct in claiming that autism screening tools have no norms for trans-identified individuals.
“[But] if you took this argument to its logical conclusion, it would be impossible to assess or diagnose anyone who identifies as transgender with anything—a learning disorder, depression, anxiety, intellectual disability and so on, because there are ‘no norms’ for them,” she said.
“It is accepted practice to use the tools you have available and to use clinical judgment and observations until new tools are created, if necessary.
“Ethically, it would be deemed a greater risk or harm to not diagnose someone, even with poor tools—it would stop kids from getting support in schools, early intervention, and [funding under Australia’s National Disability Insurance Scheme]. That would be considered discriminatory.
“The underlying brain areas impacted by autism are universal and include deficits in adaptive functioning (social skills, self-care skills), executive functioning, communication and sensory issues—regardless of gender identity.”
“The [approach of the Dutch pioneers of paediatric gender transition] differs from the [Tavistock’s] approach in having stricter requirements about provision of psychological interventions. For example, under the Dutch approach, if young people have gender confusion, aversion towards their sexed body parts, psychiatric co-morbidities or autism spectrum disorder (ASD) related diagnostic difficulties, they may receive psychological interventions only, or before, or in combination with medical intervention. Of note, in 2011, the Amsterdam team were reporting that up to 10 per cent of their referral base were young people with ASD.”—Dr Hilary Cass, interim report, February 2022
Gender change as a solution
In 2018 de-identified case notes, psychiatrist Dr Brian Ross from the Queensland gender clinic discusses the overlap between youth gender dysphoria and autism spectrum disorder (ASD).
“Individuals with ASD have the same rights as other individuals to appropriate assessment and treatment of gender-related concerns,” Dr Ross says.
He cites several possible reasons for minors with autism identifying as trans or gender-diverse, including the wish “to find a community or tribe” or the belief it will be “safer to change gender” after sexual assault.
He suggests a girl with autism might identify as a boy because she thinks “boys are logical, girls are complicated and unkind in ways I don’t understand.”
And boys with autism might identify as a girl because they are “shy, submissive and introverted, don’t like dirt on their hands, [are] vulnerable and prefer intellectual pursuits.”
Dr Ross adds a warning that “these psychosocial explanations do not explain that for a socially disabled adolescent, the choice of another gender [at] variance to their biological assigned gender could in fact worsen underlying ASD factors.”
He describes three gender clinic patients with autism—
W, a nine-year-old female. Diagnosed with autism at the age of three. Wore boys’ clothes from age of four. “Solitary non-imaginary play with a preference to be a ‘dog’ where he would bark like a dog and seek affection by rubbing himself against others like a dog.” Could not fit in with peers. Mother thought her daughter might have identified as a boy because she lacked the more advanced language and social skills of her female peers.
Mother concerned that puberty blockers might deny her child the positive effects of her natural oestrogen and “disadvantage her child’s true gender journey.” Dr Ross reassured mother that the clinic had allowed W to enter early puberty to expose the child to oestrogen and the resulting intensification of gender dysphoria favoured the early use of puberty blockers. With natural sex hormones suppressed, W would have “a better ability to explore and experience his gender identity without the distress of his gender dysphoria.”
L, a 13-year-old female. Identifies as a boy. Father diagnosed with brain tumour when she was five months old. “Observed to not socially function in a socially appropriate [way] at school or in the family.” Few friends. “Acknowledges that he is becoming socially avoidant and experiences increasing anxiety in some social situations.” Special interest in the history of Prussia and American statesman Alexander Hamilton.
Diagnosed with autism spectrum disorder (ASD) at the gender clinic after speech therapist noticed language impairments. “Delay in detection of ASD may have arisen with the preoccupation with the father’s illness and death throughout this child’s development.” L describes four personas inside her head: “C, a gay man with HIV who is angry; R, an angel-like character who is protective of all the other personas; V1, a man who likes sex; and V, who is wanting a physical form, such as his own physical body, to express himself.” Dr Ross says L presents “as a socially odd ASD transgendered adolescent who discusses his issues in the psychodrama of his various personas” but is not psychotic or suffering from dissociative identity disorder (once known as multiple personality).
S, a 12-year-old male. Initial psychology screening suggested autism features. “Wanted to be a girl because they are kinder and seem to have and hold more friends than boys that he found rejected him after a period of time… [His] desire to be a girl arose from his need to have friends and be accepted in the context of his lifelong social skills deficits and impaired social functioning… [He] was unable to articulate any other benefits of his desire to be female [and] was not able to describe any revulsion of his male body.” Dr Ross concludes that S meets the diagnostic criteria for ASD level 1 (or Asperger’s syndrome) and does not have gender dysphoria.
GCN put questions to the office of Queensland Health Minister Shannon Fentiman and Children’s Health Queensland.
There are some uncertainties in data obtained under Freedom of Information law; clinics generally do not respond to requests for clarification.
A 2019 study at the Perth gender clinic found that 18.3 per cent of a group of 104 patients showed severe autism traits on the SRS-2 measure. The researchers used scores in the severe range of this screening measure as a good enough sign of autism. They said: “Although [the SRS-2 screening tool] is not a diagnostic measure, it is effective and convenient in flagging potential [autism], which may, in turn, help to inform clinical assessment and treatment decisions, as well as prompting referral for formal [autism] assessment.” Mental health data were missing for 10.6 per cent of the patient group.
In 2020, the internationally recognised expert on Asperger’s syndrome, Tony Attwood, urged Australian authorities to establish an inquiry into the overrepresentation of teenagers with autism in gender clinics. “One of the characteristics of autism is what we call a one-track mind, and sometimes the issue of gender dysphoria (discomfort with one’s body) and changing gender becomes a special interest with a phenomenal knowledge and determination,” Professor Attwood told The Australian newspaper. He said it was vital for an inquiry and research projects to look beyond the politics and “evangelising” of trans identity in order to assess not just medical treatments but the psychological outcomes, the fortunes of former patients from the clinics, the role of social media and schools in the rising caseload, and any neurological factors. No inquiry was established.
In a 10-year audit, the Royal Children’s Hospital (RCH) Melbourne gender clinic reported that 16.2 per cent of 359 patients had a diagnosis of autism. In data released in 2019, a group of 383 patients at the RCH clinic included 29 per cent with mild to moderate autism features and 16 per cent with severe autism features.
In the Cass survey, the Queensland gender clinic says it uses the Child and Adolescent Trauma Screen during assessment.
The 2016 Strang et al guideline says that “executive function deficits [related to autism spectrum disorder or ASD] may result in concrete thinking and [a] struggle with ambiguity and future thinking, which can make assessing an adolescent’s understanding of the long-term implications of gender transition/treatment challenging. In addition, ASD-related flexibility difficulties can limit a young person’s ability to embrace the concept of a gender spectrum or that gender can be fluid; adolescents with ASD may present with more ‘black-and-white’ thinking about gender.”
The 2018 “Australian standards of care” treatment guideline issued by the Royal Children’s Hospital Melbourne says that, “For some children, a formal diagnosis of ASD can be helpful for their family and teachers in understanding their social interactions and behaviour and to find strategies to manage the difficulties they encounter.” The RCH guideline argues that “the presence of [autism spectrum disorder] with confirmation of a diagnosis of gender dysphoria should not prevent access to medical treatment where indicated.” However, this co-occurrence may require “an extended assessment period”. The guideline also says that psychosis in a patient is not necessarily an obstacle to medical intervention.
Multiple studies indicate that children with autism (viz. are on the Autism Spectrum Disorder, ASD) are disproportionally represented in gender clinic cohorts, constituting around 8% of the Gender Dysphoria (GD) clinic cohort.
The ASD cohort in the general population is between 0.5% and 1%. Meaning that the ASD GD cohort are hugely disproportionately represented in gender clinics.
Data from 48,186 autistic and possibly autistic participants in 36 primary studies were meta-analyzed. Pooled prevalence of suicidal ideation was 34.2% (95% CI 27.9–40.5), suicide plans 21.9% (13.4–30.4), and suicidal attempts and behaviors 24.3% (18.9–29.6)
For a gender clinic to be not screening for autism/ASD in their patients seems incomprehensible!
I don’t think any young people should be subjected to these interventions but young autistic patients are clearly the perfect target for this ideologically-corrupted branch of medicine for all the reasons detailed above: their difficulty thinking ahead, concrete thinking, obsessiveness and difficulty tolerating ambiguity. No wonder they’re so over-represented.
For gender clinics to simply dispense with screening is yet more evidence of the exceptionalism of gender medicine. Ordinary standards—of evidence, of thorough, impartial assessment, of ethics and of transparency —simply don’t apply. Gender medicine is “special” and only those operating within it can understand it. Outsiders should simply trust the gender gurus.