

'Told you so'
There never was good quality evidence for paediatric gender change


One of the first reviews showing the impoverished evidence base for youth gender medicine has been vindicated by England’s decision to confine puberty blockers to clinical trials.
The 2019 review published in the journal BMJ EBM—the British Medical Journal’s specialist publication on evidence-based medicine—concluded that the use of these drugs with gender dysphoric children was so poorly evidenced that it was “largely experimental” and should be confined to a formal research setting.
These findings by Oxford University’s Carl Heneghan, professor of evidence-based medicine, and his colleague Dr Tom Jefferson were amplified by The Times newspaper and a BBC Panorama program “Trans kids: why medicine matters.”
The 2019 evidence review also attracted a complaint from the online gender clinician, Dr Helen Webberley—a complaint to the BMJ which Professor Heneghan and Dr Jefferson now say was “enough to close down our work in that outlet.”
(Note: the BMJ denies this claim & cites contributions to the journal by both authors since the time of the complaint. GCN has sought clarification from Professor Heneghan. The first paragraph of this article has been edited to take account of the BMJ’s response.)
Professor Heneghan was editor-in-chief of the BMJ EBM at the time of the review; he was replaced by Professor Juan Franco in January 2021.
In her complaint to the BMJ, Dr Webberley insisted that puberty blocker drugs had “been used as a means of pausing puberty in children with gender dysphoria for 20 years and [had] been shown to be safe and effective.”
She said the authors of the BMJ EBM review demonstrated a “complete lack of understanding [of] the issues around treating trans youth and the psychological impact and mental anguish that occurs if treatment is delayed or even refused.”
Earlier this month, England’s National Health Service (NHS) confirmed it would limit puberty blockers to clinical research, “as there is not enough evidence to support their safety or clinical effectiveness as a routinely available treatment”.
The hormone suppression drugs used off-label with children who identify as trans or non-binary have regulatory approval for various conditions including prostate cancer and premature puberty, but not for gender dysphoria.
Puberty blockade with these drugs starts as young as age 10-12 in order to interrupt naturally timed but unwanted bodily development. According to international data, the vast majority of children will go on to opposite-sex hormones supposed to be taken lifelong.
Video: In the U.S. Congress, Texas Republican representative Dan Crenshaw challenges “gender-affirming” physician Dr Meredithe McNamara on the evidence for paediatric gender change. The “standards of care” referred to are low-quality treatment guidelines, such as SOC-8 from the World Professional Association for Transgender Health
‘How much harm?’
On June 16, posting to their Substack newsletter Trust the Evidence, Professor Heneghan and Dr Jefferson revisited their 2019 review of the “delicate problem” of hormonal treatments for children and adolescents who reject their birth sex.
“We found poor-quality evidence wherever we looked [in youth gender medicine], which appears to be a problem swept under the table,” they wrote on Friday.
“Evidence-based medicine, applied correctly, will eventually come up with the right answer, especially in the matter of harms that most people are uncomfortable with.
“What matters now is how many children have been harmed in the intervening four years it took NHS England to review the evidence and come to the same conclusion.”
Since the BMJ EBM review appeared, systematic reviews of the evidence base for paediatric gender transition have been undertaken in Finland, Sweden, England and the American state of Florida.
All found the evidence to be very poor, uncertain or lacking, suggesting that these medical interventions represent an experiment on children without the ethical safeguards or careful data collection of formal research.
The common policy outcome in these countries is the decision to end routine use of puberty blockers, restricting this intervention to clinical trials.
“Against the background of almost non-existent long-term data, we conclude that [puberty blocker] treatment in children with gender dysphoria should be considered experimental treatment rather than standard procedure. This is to say that treatment should only be administered in the context of a clinical trial under informed consent”—Professor Mikael Landén of the Karolinska Institute, who was part of the team that carried out Sweden’s systematic review
‘Not safe for children’
In their February 2019 review for the BMJ EBM, Professor Heneghan and Dr Jefferson highlighted flaws and shortcomings in the evidence base for trans hormonal treatment.
“Little is known about the safety profile [of puberty blockers] in the context of gender dysphoria, particularly the long-term effects, and use is based largely on the effects of treatment of central precocious [or premature] puberty,” they said.
“There are a large number of unanswered questions [about puberty blockers] that include the age at start, reversibility; adverse events, long-term effects on mental health, quality of life, bone mineral density, osteoporosis in later life and cognition.
“We wonder whether off-label use is appropriate and justified for drugs such as spironolactone [used to reduce testosterone] which can cause substantial harms and even death. We are also ignorant of the long-term safety profiles of the different [opposite-sex hormone] regimens.
“The current evidence base does not support informed decision-making and safe practice in children.”
In the BMJ print edition for 6 April 2019, Professor Heneghan said there was “a complete evidence void in this area” of medication for gender dysphoria in minors.
“It’s one of the poorest bodies of evidence I’ve ever seen to inform decision-making in a field,” he said.
“There are no clinical trials, there are no randomised controlled trials, we only found two studies that actually used case-control methods.
“This approach to medicine, which says that we can just use drugs because we think they’re a good idea or because patients want them, is difficult for me to rationalise as appropriate.”
“One of the first medical organizations to encourage gender transitions for young people is holding its annual meeting here [in Chicago]. It’s called the Endocrine Society, and while few people have ever heard of it, it has shaped the highest levels of policy since 2017. While European countries are rapidly pulling back from these [paediatric gender] treatments, based on growing evidence that children are suffering, America continues to promote them based on the society's endorsement”—endocrinologist Dr Roy Eappen, senior fellow at Do No Harm, Daily Herald, 16 June 2023
‘Go with guidelines’
In her complaint, Dr Webberley of the online clinic GenderGP claimed that the BMJ EBM review “provides an unbalanced view, cherry-picks and is often factually incorrect.”
An update note on the review said a correction was made to one statement about a study (a missing “not”). Under “Competing interests”, the journal stated that the review was carried out as part of the Panorama program.
Dr Webberley had faulted the review for not giving weight to international treatment guidelines which she said were “evidence-based” documents that “[acknowledged] the quality of available evidence when making recommendations.”
She cited guidelines from the World Professional Association for Transgender Health (WPATH), the Endocrine Society and the Royal Children’s Hospital Melbourne (RCH).
The first two guidelines have not measured up to the standards of evidence-based medicine, according to a BMJ investigation.
And one of the pioneers of evidence-based medicine, Professor Gordon Guyatt, has declared the RCH guideline untrustworthy because of its failure to grade the calibre of evidence supposed to support its treatment advice.
“When I’m in a cynical mode, I sometimes joke around and say, ‘If you don’t do research, you write guidelines’ ”—Dr Ken Zucker, international expert on youth gender dysphoria, The Australian, 22 October 2019
Gender expertise
The day after NHS England announced that puberty blockers would be restricted to clinical trials, Dr Webberley said the news was “making people fearful and sad. Sad that their child won’t get the care they need in time. Sad that their child will be forced into research projects against their will.”
On her website she set out her view of how care should be delivered, again recommending gender-affirming guidelines including those from WPATH, the Endocrine Society and RCH.
She said puberty blockers “prevent the person from developing secondary sex characteristics that do not match their gender identity.
“They prevent boys from menstruating and having gynaecomastia and they prevent girls’ voices from breaking and from growing beards and moustaches and size 12 feet.”
Gynaecomastia, often referred to as “man boobs”, is the enlargement of male breast tissue, but Dr Webberley was referring to girls who identify as boys.
She argued that the new cautious approach by the NHS was “harmful, dangerous and discriminatory,” and had no effect “on private doctors and what they decide is the right care for their patients.”
In March, Dr Webberley won a court appeal against her suspension for serious misconduct in allegedly not discussing the fertility risks before starting an 11-year-old female patient on puberty blockers.
“Today marks the day where I am free to practise in my profession again,” she said.
The misconduct case against Dr Webberley had its origins in concerns raised by several clinicians at the London-based Tavistock youth gender clinic about the online care given by GenderGP to patients also being seen at the Tavistock or on its waiting list, according to BBC journalist Hannah Barnes in her book on the collapse of the Tavistock clinic.
What kind of expertise?
After I reported the findings of the 2019 BMJ EBM review in The Australian newspaper, the RCH gender clinic director, Dr Michelle Telfer, lodged a complaint on the grounds that Professor Heneghan was not a gender expert and had been criticised in Oxford University’s student paper, which quoted activists as saying “his words attempt to give credibility to a transphobic rhetoric”.
As Professor Heneghan and Dr Jefferson explained in their June 16 Substack post, they began with the treatments recommended by WPATH guidelines and “then proceeded to do what we do for a living: look at the evidence from systematic reviews, focussing on the most up-to-date and most of all, we looked at the quality of the 16 studies in the reviews.”
Graphic: In the discipline of assessing the quality of evidence, systematic reviews of the scientific literature far outrank treatment guidelines reflecting the “expert opinion” of any group of specialists, such as gender-affirming clinicians
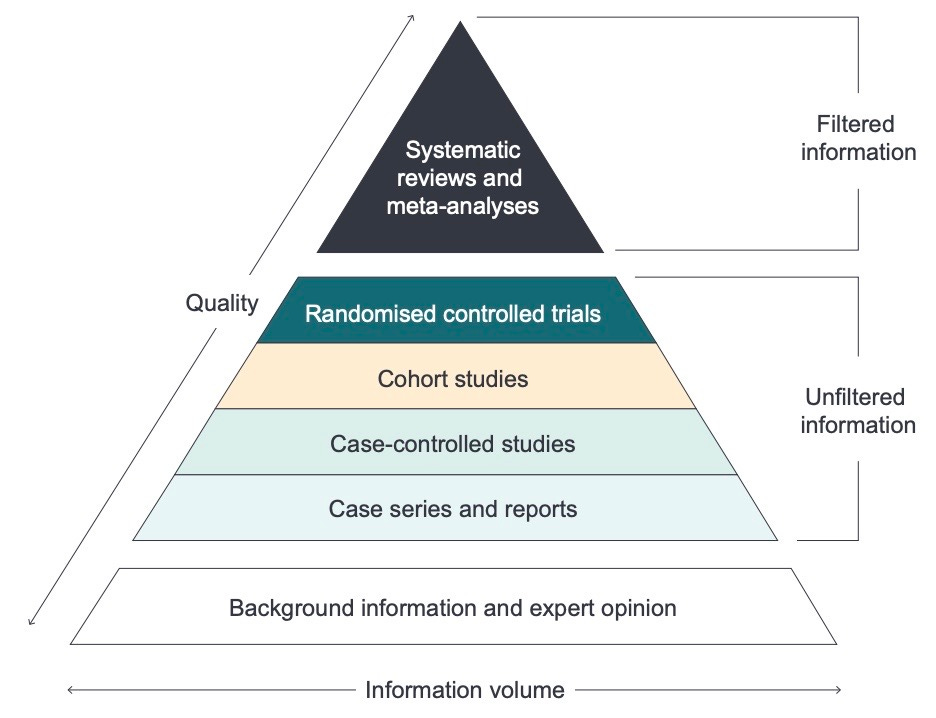
Note: GCN sought comment from Professor Heneghan, the BMJ and Dr Webberley. RCH has defended its treatment guideline as “peer reviewed at the highest level, published in the Medical Journal of Australia and adopted by healthcare providers across Australia and the globe”
I would love to be a fly on the wall at the sociologist’s conference 50 years from now. They will surely wonder “how on earth did this happen?”. How, on the basis of a metaphor taken literally (the born in the wrong body myth) by gullible or opportunistic doctors, and promulgated throughout society including to kids by a rapacious industry rich enough to buy politicians and institutions, were so many children’s bodies and futures damaged beyond repair.
As now stood-down heretic Qld psychiatrist Jillian Spencer pointed out in her recent YouTube video on models of care for gender dysphoria, historically the concept of “therapeutic collusion” was taught to all psychoanalysts. The point was to avoid colluding with a patient’s self-serving or delusory worldview, despite this being a tempting way to avoid dealing with uncomfortable facts, to relieve the patient’s and the therapist’s anxiety and to build a false rapport—all to the patient’s ultimate detriment. Gender doctors have clearly never heard of the concept, as we can see from some of the bizarre-bordering-on-psychotic comments made by one of the medicos quoted above. Collusion has been renamed “affirmation” and is now essentially mandatory.
There has been a longstanding failure to train medical students in the scientific method, according to physician and addiction specialist, Dr Drew Pinksy, who spoke about this during his recent chat with Gad Saad on the latter’s podcast show The Saad Truth. This is obvious when we see gender doctors defending their trade by resorting to emotive pleas and citing physician consensus rather than evidence. Now that medical training has been overtaken by indoctrination in “identity”-driven social justice narratives, this ignorance about what constitutes meaningful evidence and the failure to understand the principle of “do no harm” can only deepen.
The rationale used to justify extreme invasive mutilating off-label, ‘no-way-back’ therapies is, at times, appropriate in the heroic corner-cutting off-label efforts that are justified in otherwise disastrous terminally fatal medical conditions.
Yet here we are applying them to otherwise healthy children and young folk.