
Time's cure
How many of today's young patients will simply outgrow the distress of gender dysphoria?


Parents may be disappointed if they assume that most of today’s young patients with gender dysphoria will benefit from the past’s high rates of resolution without medical intervention, according to clinical psychologist Dr Ken Zucker, who is an international authority on this condition of distress in the sexed body.
The claim is often made that hormonal and surgical treatments are an unnecessary risk because the vast majority of transgender-identifying young people will grow out of gender dysphoria and reconcile with their biological sex. Multiple follow-up studies dating back several decades show this phenomenon known as desistance.
A frequently cited 2021 paper by Toronto University psychologist Dr Devita Singh and colleagues reported that 87.8 per cent of 139 boys outgrew their childhood-onset gender dysphoria. The mean age at follow-up was 20.6 years. Comparable rates of desistance have been documented by Dutch researchers (79.7 per cent in Wallien 2008, 70.9 per cent in Steensma 2013).
However, Dr Zucker, who is a key researcher in the desistance literature, said he believed it was a mistake for parents to apply the outcomes of dysphoric children first seen by specialist clinicians in childhood to today’s distinct group of under-researched patients first seen in adolescence.
“You’re sort of making an assumption that, ‘Oh, there’s going to be an 80 per cent desistance rate, so why would I put my kid on hormones’,” he said in an interview with GCN.
“I’ve had many discussions with parents about that parameter over the years, and I often feel that my argument never sinks in—I don’t even know if it gets in the first ear.
“It’s not necessarily an argument for going down the medical path.”
“I have met many parents in the course of my work who thought that their teen wouldn’t medically transition because of the 80 per cent desistance rate. But this desistance literature is mostly from a different cohort and certainly from a different time”—psychotherapist and Genspect director Stella O’Malley, email to GCN
Case-mix flip
The desistance literature involves children, mostly boys, from the era before the acceleration of social media and before the emergence, since the 2010s, of an unprecedented number of chiefly female teenage patients, an age and sex profile at odds with classic gender dysphoria. Today’s adolescent patients often have no known childhood history of gender distress.
The desistance studies also predate the pervasive influence of the “gender-affirming” treatment model with its championing of social transition before onset of puberty, whereby the child is enabled to live out a trans or non-binary identity alien to biological sex.
Another relatively new factor is the promotion of early access to puberty blocker drugs, with the limited data available showing the vast majority started on blockers go on to cross-sex hormones making them lifelong medical patients.
Dr Zucker, a Toronto-based clinician who edits the journal Archives of Sexual Behavior, said he believed the persistence rate—the proportion who do not outgrow gender dysphoria—would be “way higher” for today’s patients first seen in adolescence, compared with outcomes for those first seen in childhood before onset of puberty.
He cited several reasons for this view—
some patients seen for the first time as adolescents will have had persistent dysphoria since early childhood
young children—say, at age 5—offer a wider developmental window for therapy
today’s patients seen first as teenagers may already have socially transitioned away from their biological sex, making persistence of gender dysphoria and medical intervention more likely
early social transition, itself an intervention with psychological and social implications, was thought to be rare in the period covered by the desistance literature
the relatively recent growth of “gender minority subculture” online
the new practice of schools enabling the social transition of students without parents being told
Dr Zucker said today’s adolescents seen by clinicians for the first time would include a large number of patients fitting the “rapid-onset gender dysphoria” (ROGD) term coined by the public health researcher Dr Lisa Littman.
“We really don’t know yet what percentage of the ROGD [patients] are going to persist—it’s not going to be 100 per cent, but it’s not going to be zero, either,” he said.
The ROGD hypothesis is built on parent reports of young people suddenly disavowing their biological sex, with this gender distress emerging for the first time during or after puberty in the context of online immersion and peer influence.

Cease and desist
Both Dr Zucker and Dr Littman were among the presenters at The Bigger Picture conference staged by Genspect in Ireland and online from April 27-29.
On Friday Dr Littman told the audience that a new study of desisters (those who cease to identify as transgender before any medical intervention) and detransitioners (who stop medical transition and may re-embrace their biological sex) was undergoing peer review.
She said this study embraced young adults aged 18-33 who became teenagers after the “more lax” standards of care issued in 2011 by the World Professional Association for Transgender Health.
“It’s a cohort that experienced social media growing up, and we asked them not just about factors associated with becoming trans-identified and becoming not-trans identified, we asked them to rate [these factors] in importance,” she said.
She said detransitioners in this study who did not go back to tell former clinicians they had ceased trans medical treatment were asked their reasons. (Her 2021 survey report of 100 detransitioners found that only 24 had informed the clinicians who had enabled their transition.)
Graphic: Systematically speaking
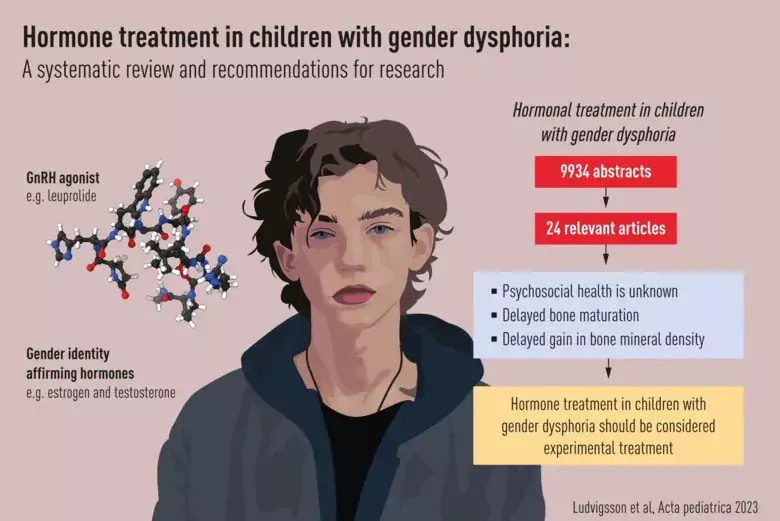
“Our [systematic review of the evidence for hormonal treatments] is important not only because the incidence of young people with gender dysphoria has increased during a short period of time, but also because of the change in [patient] case-mix”—psychiatric researcher Professor Mikael Landén of Sweden’s Karolinska Institute and University of Gothenburg, media statement, April 2023. He is one of the authors of a new journal article based on the systematic review that led to Sweden adopting a more cautious approach to gender medicine in 2022.
“We do not know what the natural trajectory is for these children. Studies should first elucidate to what extent gender dysphoria spontaneously remits in adolescents who have not presented gender incongruent behaviour in childhood. If predictors for persistence can be found, the second step would be to conduct clinical trials focusing on potential persisters in order to evaluate the beneficial and adverse effects of hormonal treatments. Importantly, such studies need to follow patients for many years.
“Against the background of almost non-existent long-term data, we conclude that [puberty blocker] treatment in children with gender dysphoria should be considered experimental treatment rather than standard procedure. This is to say that treatment should only be administered in the context of a clinical trial under informed consent.”
Video: Detransitioners’ Q&A panel discussion
Leading indicator
In Finland, a pioneer of youth gender medicine which in 2020 stopped routine paediatric transition and gave priority to psychiatric and social interventions, there are tentative signs of an interesting outcome, according to the prominent clinician and researcher Professor Riittakerttu Kaltiala of Tampere University Hospital.
“My clinical impression and our very preliminary observations on hospital statistics suggest that a majority of those adolescents who cannot be recommended for medical transition in the gender clinic—mainly because of untreated psychiatric disorders—seem to desist later,” Professor Kaltiala told GCN.
“But it is too early to say anything for sure—all the assessed patients are still less than 30 years old.”
For today’s childhood-onset cases of gender dysphoria, she sees no new evidence that would rule out the high desistance rates of the past if the traditional “watchful waiting” approach were used. (This is a more cautious treatment approach than the gender-affirming model.)
Last year, a study of social transition and gender identity by Princeton University psychologist Dr Kristina Olson was hailed as proof of the gender-affirming mantra that trans kids are experts in their identity.
The research was reported by The New York Times with the headline “Few Transgender Children Change Their Minds After 5 Years”. (The Olson study lacked a comparison group of gender dysphoric children who were not socially transitioned.)
Professor Kaltiala regards the study as an unintended vindication of the more cautious watchful waiting approach with distressed children who are yet to begin puberty—an approach open to the likelihood of desistance.
“In this study by Olson et al, the children were actively [socially] transitioned. When this was done, they did not desist,” she said.
“Given the earlier evidence [of the desistance literature] this shows that active transitioning—socially and medically—of the children likely keeps them on the trans-identity path [at least into adolescence].
“[But] it is not yet known whether the outcome of these social and medical transitions will be good, because all published follow-up studies are of very short duration.”
“If anything, these findings [such as Olson’s] send a strong warning that the decision to proceed with early paediatric transition actually forecloses on the possibility of the child achieving a resolution of gender dysphoria as he or she gets older, and thereby solidifies the young person as a permanent medical patient”—licensed professional counsellor Sasha Ayad, email to GCN
“A gender social transition in prepubertal children is a form of psychosocial treatment that aims to reduce gender dysphoria, but with the likely consequence of subsequent (lifelong) biomedical treatments as well (gender-affirming hormonal treatment and surgery). Gender social transition of prepubertal children will increase dramatically the rate of gender dysphoria persistence when compared to follow-up studies of children with gender dysphoria who did not receive this type of psychosocial intervention and, oddly enough, might be characterised as iatrogenic [medical treatment causing illness]”—Dr Ken Zucker, journal article, 2019
Not a cure-all
Professor Kaltiala said the outcomes in Finland of cross-sex hormone treatment begun in adolescence were not encouraging.
In a 2019 paper, she reported that this treatment was “not enough to alleviate psychiatric co-morbidities, which in adolescents with gender dysphoria may also precede gender identity concerns”.
Nor was functioning in education and work improved by gender dysphoria treatment.
“Difficulties in school adjustment and learning are common among gender-referred adolescents and often not properly addressed, on the assumption that treatment of gender dysphoria would relieve an array of problems,” her study said.
Psychiatric disorders and difficulties with peers, schooling and work life all demanded specific interventions, a conclusion at odds with the gender-affirming approach and its tendency to suggest that transition will resolve myriad problems.
“The 80 per cent [desistance] figure comes from the follow-up studies of early/pre-pubescent onset cases. It doesn’t generalise to adolescent onset. Also, the [early-onset] kids were in therapy at the same time. We can’t really predict the outcomes for teens who are instead receiving whatever social and online pressures saying trans is cool”—clinical psychologist and sexologist Dr James M. Cantor, email to GCN
“The watch-and-wait [or watchful waiting] approach is only pertinent to childhood-onset cases in the sense that the follow-up studies on childhood-onset cases show that most but not all desist. We have no such evidence for the adolescent-onset cases, not because the evidence shows different outcomes, but because there have not been any follow-up studies of them at all.
“The lack of evidence of desistance does not mitigate against watch-and-wait, however. Watch-and-wait is the correct policy exactly because we have no evidence: in medicine we do nothing, and in science we stick to the null hypothesis, until after we have evidence of potential benefit and lack of potential harm.”
Adolescent therapist Sasha Ayad, co-presenter of the podcast Gender: A Wider Lens, said adults had to be careful how they responded to a child experiencing gender distress.
“It’s wonderful that gender non-conforming young people have found greater societal acceptance, but when teachers, peers and other adults in the child’s life confirm their identity, this goes beyond non-judgement to psychosocial intervention,” she told GCN.
“In such an aggressively affirmative environment, I find it unlikely that a young person would be able to question and move through identity exploration without being nudged in only one direction—that of social and medical transition.
“Therapists should emphasise that publicly changing one’s identity, while sometimes described as a neutral and reversible exploration, is actually a psychosocial intervention that creates a reciprocal process by which the young person assumes a gender identity and the world around him or her confirms it.
“This is likely to make it more challenging for the young person to change his or her mind, due to the power of positive encouragement and reinforcement which exists in overly-celebratory pro-transition environments.
“Even if the young person comes to feel social transition wasn’t really the best choice, the desire to save face in front of peers and other young people is hard to contend with. After spending such a tremendous effort convincing everyone to go along with the new gender, it would be so difficult to admit you were wrong. The sunk cost fallacy seems apt in these cases.”
Detransitioners as guides
“Unfortunately we do not have a study of adolescents who were left without intervention. The dilemma is that since the onset of ROGD, access to puberty blockers has been almost universal, at least until people realised that very few girls changed their minds and almost all proceeded to cross-sex hormones”—child psychiatrist and founder of the Toronto youth gender clinic Dr Susan Bradley, email to GCN. (Dr Zucker was her colleague at the Toronto clinic and followed her as director.)
“We wondered when we first used these blockers [at the Toronto clinic] whether we were in fact encouraging the transition as opposed to buying time [for patients to explore their identity and treatment options]. We also were made to understand that the blockers were completely reversible and caused no long-term effects.
“We now know that that information was not accurate and with the more recent finding of almost universal transition to cross-sex hormones, we realise that blockers act almost like a gateway drug.
“The thing that has made clinicians jump on the puberty blocker train is the worry about suicide. This is a group who often have suicidal feelings, but these are often fleeting and they continue even after transition.
“The social contagion of ‘being trans’ that we have seen would really indicate that it is highly unlikely that most of these teens are in the group of ‘true transsexuals’, if there is such a thing. Some of the articulate detransitioners make this pretty clear.
“At this point, all we can say is that the evidence base is not there.
“I believe that in the absence of good science, we need to be guided by what we are hearing from detransitioners, many of whom have indicated that they should not have been allowed to make the decision to go on blockers without a lot of help to understand where these ideas [driving the wish to transition] have come from, and to explore other options that are safer.”
Thank you!
My 2 cents from watching--it's not clear from the earlier cohort what is going to happen to the young people of this new group who do go on hormones, if they are doing it for the wrong reason (if their gender dysphoria is being driven by other issues). Even some of the initial kids who persisted are now recognized as having been autistic or having separation anxiety, both things which therapists are now better understanding can lead a person to seize onto transition as the solution to their distress. And people are learning ways to support this separation anxiety and these autistic traits without transition now. Someone asked about this at the Genspect conference--don't we know more about how to support even the young kids? It seems so. Unfortunately, the wave of enthusiasm for the young people to just medicalize is doing them enormous harm.
For those who have seized upon a concrete solution to a mental health struggle, a developmental struggle, medical transition is not a solution, as the issues still remain, and the drugs and surgeries wreak physical havoc, their bodies will keep fighting the drugs and trying to flush them out of their systems. So maybe they won't all desist, but maybe some will transition and then realize they were being "led" as O'Malley says. Many people say they eventually realize they aren't going to turn into the other sex. It might give them time to grow up and deal with their problems, but the health problems, especially if surgery is involved, are incredibly serious.
Ironically, there is currently a stigma around mental health support--they're given a choice of get to know yourself and deal with reality, which is scary and, given how hard these kids are on themselves, threatening, or take on the role of being trans, being treated as special and being able to duck out of some of the parts of growing up, for now. But they will grow up, anyhow, and then....I just hope our society in general will begin to welcome them to be their authentic selves when it doesn't involve them constantly taking drugs to do so. Not like now. The kids having trouble moving back....we can help with this. The MD's into "genderfluid" should be encouraging kids to be fluid back into "not trans at all" rather than telling them they're transphobic when they realize that might be the case for them, which is what many people are reporting.
I don't understand why these interventions are being offered outside of experimental safeguards. 55 kids....really?
The rate of Desistance in children diagnosed with Gender Dysphoria is dependent on whom you ask. One side of the equation states ‘never/rare’ the other ‘frequent’.
Not surprisingly both sides of the equation are convinced of they are correct and clearly one of them is not.
The logical fallback in interventional medicine is the age-old adage of ‘do no harm'.
A medical intervention involving children and young people that includes irreversible hormonal and surgical mutilation rings a lot of ‘harm’ bells, all the more so given that there is a distinct possibility that the reason the intervention may well have been transient.