
Strong drugs, weak evidence
Lack of long-term safety data puts gender clinics in a bind

The gist
Gender clinics giving children and teenagers puberty blocker drugs and cross-sex hormones cannot wait for long-term data on the safety of these interventions, according to an editorial in the medical journal BMJ.
“It will take many years to obtain these [undoubtedly needed] long-term data,” says the article, which has Dr Ken Pang, head of research at Australia’s largest children’s hospital gender clinic, as lead author.
The BMJ-commissioned editorial argues there is enough existing evidence and international agreement among gender clinicians to continue these medical treatments aimed at stopping unwanted puberty, then mimicking opposite-sex development.
The Pang article, published on April 1, is a critical response to last month’s interim report from the United Kingdom’s Cass review.
Dr Hilary Cass, a former president of the Royal College of Paediatrics and Child Health, is leading the independent review of treatment for minors diagnosed with gender dysphoria, a distressing sense of conflict between birth sex and an inner “gender identity”.
The interim report, informed by systematic reviews of the medical literature, says “gaps in the evidence base” prevent, at this stage, any “definitive advice” on the use of puberty blockers or cross-sex hormones. This lack of advice is “problematic [and] a disappointment”, the Pang BMJ article claims.
The Cass report says there is only “limited” longer-term follow-up data on what happens to patients of gender clinics — both internationally as well as within the UK.
The background to the Cass review is the saga of England’s Tavistock youth gender clinic, with concerns including a surge in atypical gender dysphoria cases, medicalisation, poor data collection, failures in safeguarding, and litigation brought by a former patient, Keira Bell, who started puberty blockers at age 16.
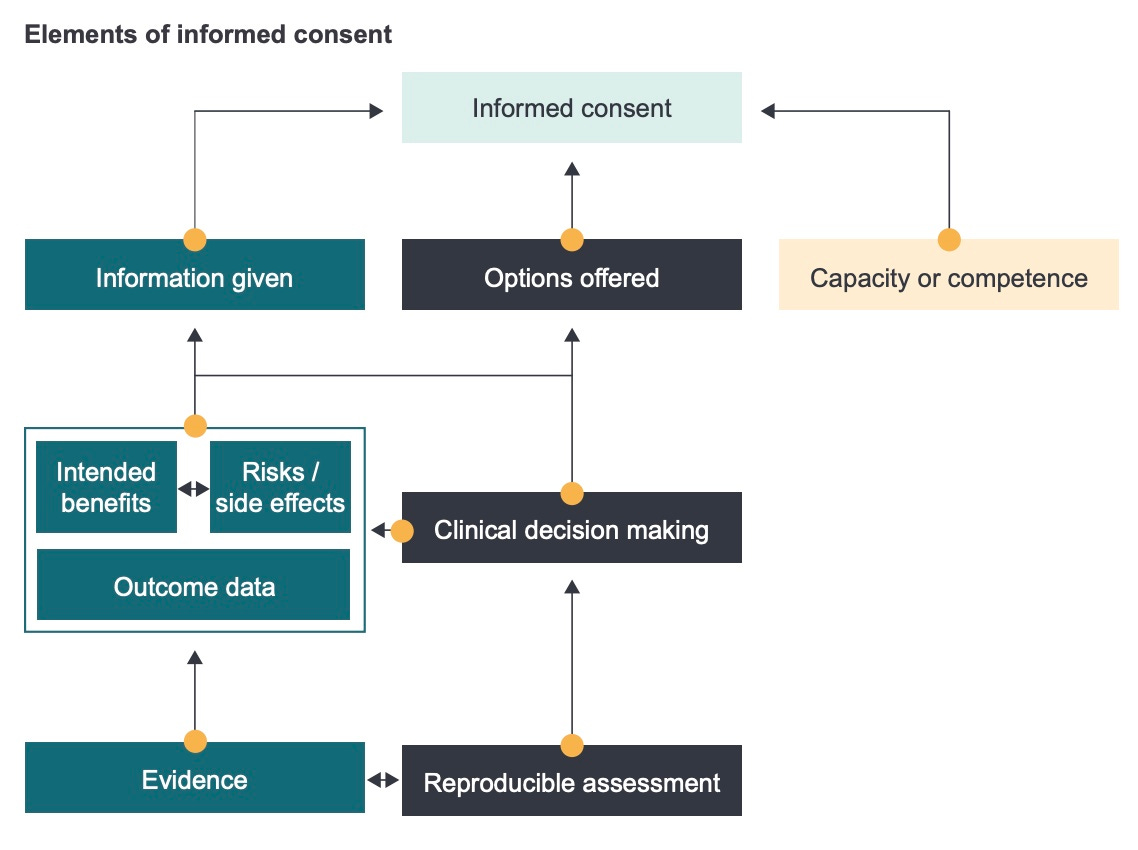
The interim Cass report says puberty blockers, first used for gender dysphoria by a Dutch clinic in the 1990s, involve more uncertain outcomes than cross-sex hormones, making it crucial for clinicians to document “fully informed” consent before a child’s natural development is suppressed.
In a BMJ opinion article last month Dr Cass notes concerns about the widely used “gender affirming” treatment approach, in which a child’s self-declared transgender or non-binary identity is typically “affirmed” by clinicians, parents and schools.
Some clinicians in primary and secondary care told the Cass review they felt unable to carry out the proper assessment and differential diagnosis of normal clinical practice because “an unquestioning affirmative approach” was expected.
Disagreeing about consensus
Under the headline “Landmark review should interrogate existing international evidence and consensus”, Dr Pang’s BMJ article claims that the Cass report “ignores more than two decades of clinical experience as well as existing evidence showing the benefits of these hormonal interventions on the mental health and quality of life of gender diverse young people”.
The article says the report “curiously” makes “little or no mention” of the clinical consensus represented by treatment guidelines and position statements — endorsing the gender affirming approach and medicalised gender change — issued by the American Academy of Pediatrics, the Endocrine Society, and the World Professional Association for Transgender Health (WPATH).
Dr Pang and his Australian colleagues suggest the UK and its Tavistock clinic are out of step with agreement elsewhere in the world that hormone suppression is best begun early in puberty.
The Pang article does not mention last year’s dramatic interventions in the international debate by three prominent US gender clinicians — past and present leaders of WPATH — whose concerns include the early use of puberty blockers, skyrocketing demand by teenagers for medical interventions, and sub-standard assessment.
American clinician and researcher Dr Diane Chen, the founding psychologist of the gender and sex development program at Lurie Children’s Hospital of Chicago, said in a recent interview with Undark Magazine that she believes “a lot of the questions around long-term medical health outcomes we won’t be able to answer until the youth who started hormones at 13, 14, 15, are in their 50s, 60s, 70s”.
However, psychiatrist and researcher Dr Annelou de Vries, from the Amsterdam clinic which pioneered the use of puberty blockers as the first of a three-stage process of medical transition, told GCN she agrees with Dr Pang that there is “considerable consensus” about these interventions, and that “evidence alone will not provide the answer”.
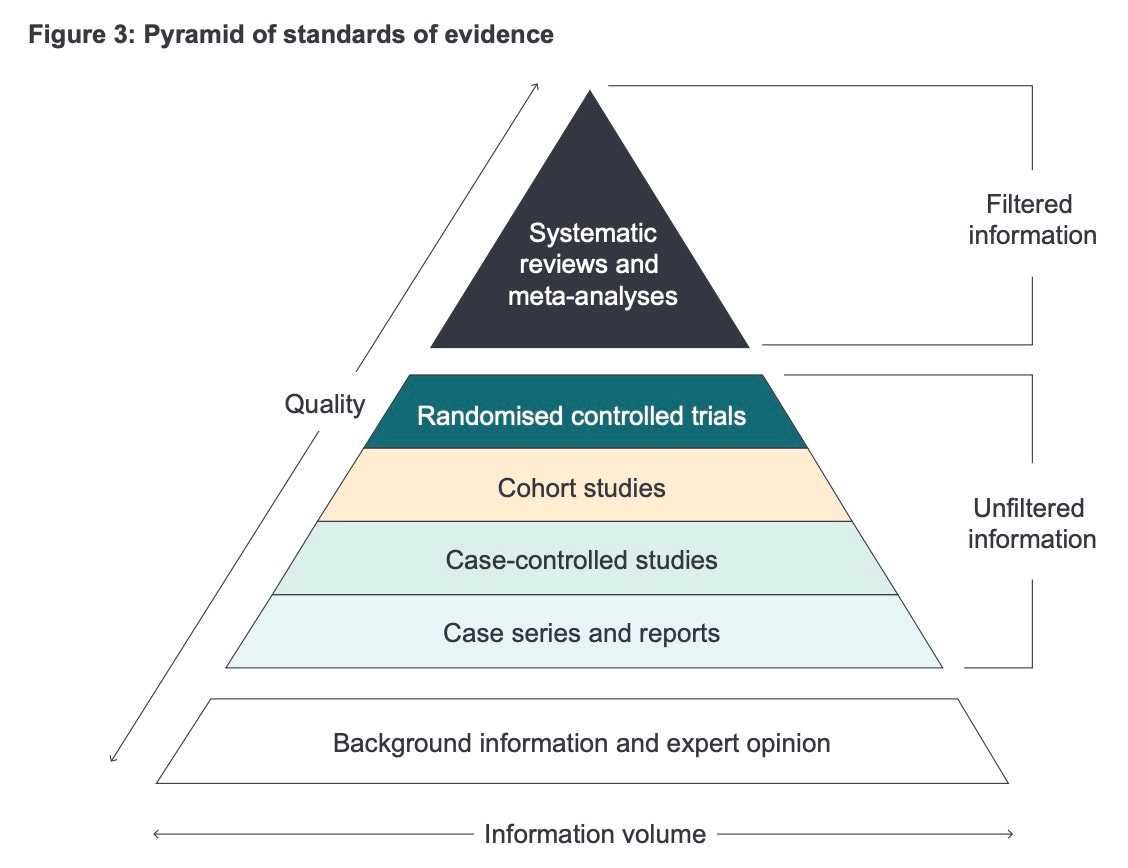
Within evidence-based medicine, clinical consensus about treatment may be regarded as an inferior substitute for good scientific evidence.
In an open letter to young people worried they will be denied medical interventions, Dr Cass says: “Whenever doctors prescribe a treatment, they want to be as certain as possible that the benefits will outweigh any adverse effects so that when you are older you don’t end up saying ‘Why did no-one tell me that that might happen?’.”
The detail
NICE work
Both the interim Cass report, and the October 2020 systematic reviews by the UK National Institute of Health and Care Excellence, refer to the weak state of evidence internationally, not just in the UK.
In its search of the medical literature for evidence on puberty blockers, NICE found 525 references, but after screening for quality, only nine studies were included in the 2020 review. Even with these studies, the results were rated as “very low certainty”.
“A key limitation to identifying the effectiveness and safety of [hormone suppression] for children and adolescents with gender dysphoria is the lack of reliable comparative studies [involving no treatment or alternative treatment],” NICE says.
For cross-sex hormones, the NICE literature search turned up 1,997 references, but only ten qualified for the review, including two studies cited by the 2022 Pang BMJ paper as “showing the benefits” of hormonal interventions. Again, even the results of this select group of “less weak” studies were rated as “very low certainty”.
Whose consensus?
American paediatrician Dr Julia Mason, one of the authors of a new paper on doubts about informed consent to gender medicine, said she was struck by Dr Pang’s article claiming an international consensus on the strength of three US-dominated treatment guidelines.
Dr Mason says the BMJ article overlooks Finland’s 2020 decision to set aside the WPATH guideline and to recommend psychotherapy as the first-line treatment for dysphoric youth, rather than hormonal treatments with a weak evidence base.
She says Sweden’s National Board of Health and Welfare rightly concluded earlier this year that “the risks of hormonal treatment for those under 18 outweigh the benefits, and that these interventions should not be offered outside of clinical trials”.
Interview: Munich psychiatrist Dr Alexander Korte on the challenge of puberty —and its necessity for identity formation.
Poor guidance
The 2011 guideline from WPATH has been criticised as lacking in rigour. The Endocrine Society’s 2017 advice on hormonal treatment of adolescents is based on data rated as “low quality” or “very low quality”.
Neither document rises to the level of a “standard of care” because gender medicine “is far from settled science”, according to American endocrinologist Dr Will Malone of the Society for Evidence based Gender Medicine.
The 2018 position statement from the American Academy of Pediatrics recommends the gender affirming approach with young people. It does this by misrepresenting key studies which “repeatedly endorsed [the more cautious approach of ] watchful waiting”, according to a 2019 paper by psychologist Dr James Cantor.
The WPATH and Endocrine Society documents are also cited to support a 2018 Australian treatment guideline promoted as “the world’s most progressive” and the first specifically for children and teenagers with gender dysphoria.
This document was issued by the Royal Children’s Hospital Melbourne, home to Australia’s most influential gender clinic.
The director of that clinic, Dr Michelle Telfer, is a co-author, along with her colleague Dr Pang, of the BMJ editorial finding fault with the Cass report.
Dr Telfer and Dr Pang are both authors of the RCH treatment guideline, which is badged as “Australian standards of care”.
The guideline parts ways with the practice of setting minimum ages for treatment, and advises a start to hormone suppression early in puberty (at the level of development known as Tanner stage 2-3, or roughly age 9-13).
In a 2021 paper reporting a 10-year audit of patients at the RCH gender clinic, researchers reveal that pubertal status “was not always uniformly documented in the clinical notes” and therefore age was used as a proxy for Tanner stage in the audit.
The RCH treatment guideline claims that “chest reconstructive surgery” [mastectomy] is “regularly performed” at age 16 in countries where that is the age of majority, and argues that psychosis or depression in a minor “should not necessarily prevent medical transition”, although this might complicate clinical decisions.
The guideline states that its recommendations are based “primarily on clinical consensus”, the WPATH and Endocrine Society documents, and “a limited number of non-randomised and observational studies”.
The RCH guideline was considered by Australia’s National Health and Medical Research Council for inclusion in its online portal of clinical practice guidelines but did not qualify, in part because it did not include an evidence base for its recommendations.
The RCH guideline has lost its 2019 endorsement by the Royal Australian and New Zealand College of Psychiatrists, which in 2021 shifted to a more cautious approach on gender dysphoria. Gender dysphoria is a condition in psychiatry’s diagnostic manual, the DSM.
Also in 2021, a challenge to the gender affirming approach in Australia emerged in Sydney with an internationally significant paper from researchers associated with The Children’s Hospital at Westmead.
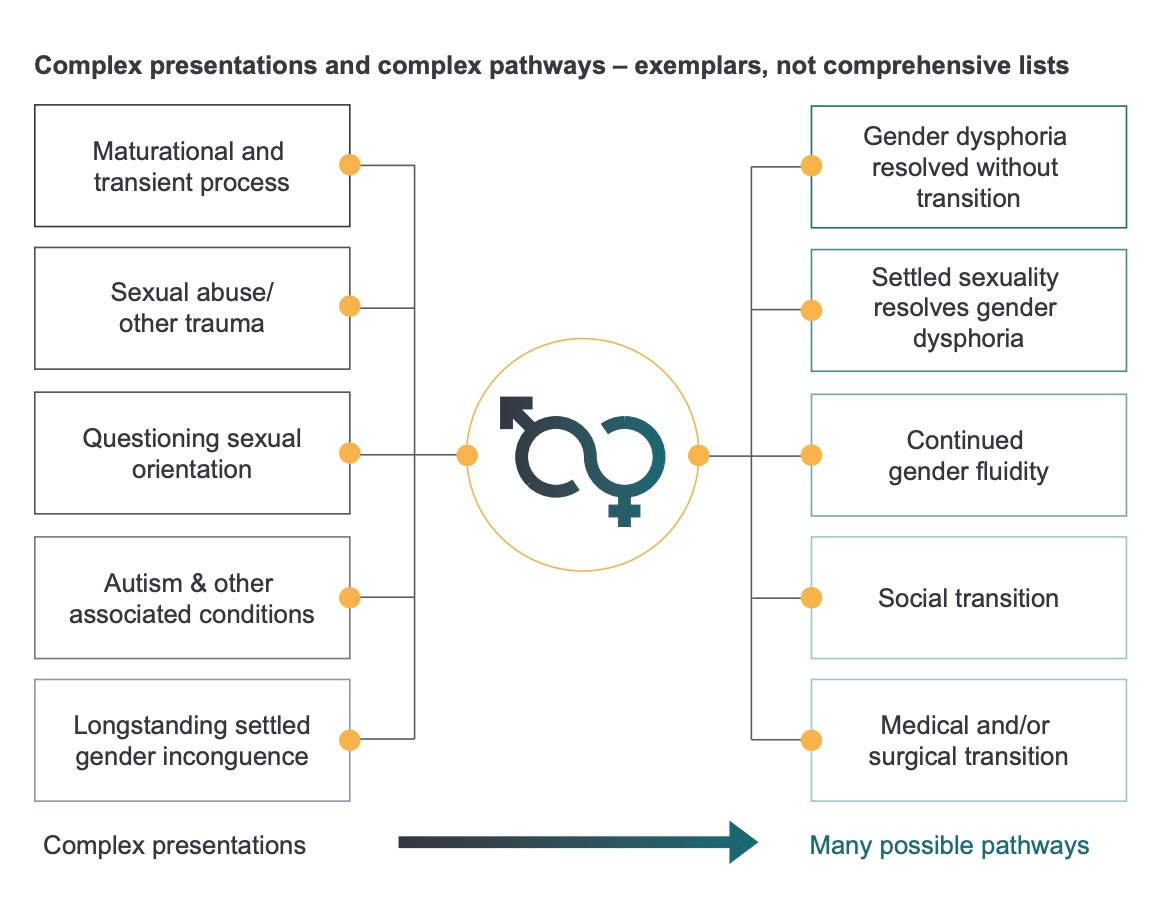
This Westmead paper warns that health professionals are under pressure to enable “conveyor belt” medicalisation of children who arrive at the gender clinic already convinced that hormonal drugs are the only solution to their distress.
At the Westmead clinic, patients had high rates of anxiety, depression, suicidal ideas, behavioural disorders, autism, and “adverse childhood experiences” such as family conflict, exposure to domestic violence, parents with mental illness, loss of important figures through separation, and bullying.
The Westmead researchers note the gender affirming recommendations of WPATH and the Endocrine Society, but make the point that “despite the existence of guidelines, the evidence base for all aspects of treatment was and remains sparse”.
They urge a shift to a more comprehensive “trauma-informed model of mental health care for children presenting with gender dysphoria”.
Impressive job
The interim Cass report notes that short-term studies claim mental health benefits from puberty blockers, but says there is “very limited research on the sexual, cognitive or broader developmental outcomes”.
Gender clinicians often acknowledge lower bone density and reduced height as side-effects of a chemically interrupting puberty, but there is increasing concern about the less familiar question of risks to the cognitive and psychological growth of adolescence.
The Cass review has a research program to plug gaps in the evidence — augmented by professional consensus where necessary — but investigation of the neurodevelopmental effects of suppressing the natural hormones of puberty has hardly begun internationally.
In a 2019 open letter, clinical psychologist Dr Kirsty Entwistle, who had worked at the Tavistock satellite clinic in Leeds, said she was troubled by clinicians telling children and families that puberty blockers were “fully reversible”.
“The reality is no one knows what the impacts are on children’s brains, so how is it possible to make this claim?,” she wrote.
“It is also a problem that [Tavistock] clinicians are afraid of raising their concerns for fear of being labelled transphobic by colleagues.”
Dr Entwistle told GCN she was “impressed” by the interim Cass report with its grasp of complex subject matter.
“I continue to hope that the [Tavistock clinic] management will be held accountable for their failures,” she said.
Incomparable treatment
The Royal Children’s Hospital Melbourne — home to two authors of this month’s BMJ editorial critical of the Cass review — has launched its own longitudinal study of gender patients, Trans20.
In the 2019 protocol paper for this 20-year study, researchers including Dr Pang and Dr Telfer acknowledge there is “little empirical data” on today’s young patients and they flag “an urgent need for more evidence to ensure optimal medical and psychosocial interventions”.
They say treatment specific to children and adolescents is “relatively new”, and clinicians need “more empirical data” on areas such as “risk and protective factors and the long-term safety and outcomes of different forms of medical interventions”.
Trans20 does not use an untreated control group nor a comparison group given alternative treatment to the gender affirming model, such as the “watch and wait” approach.
This could undermine any confident claim that positive outcomes for patients in the study demonstrate the effectiveness of gender affirming interventions (although the researchers say that, “where possible”, measures with population-based data will be used for comparison).
As part of the Trans20 study, which began recruiting patients in 2017, RCH’s research partner the Murdoch Children’s Research Institute advertised a PhD project under the title “Influence of pubertal hormones on brain development.”
The PhD project description says it’s “likely” that the naturally occurring hormones of puberty “play an important role” in the rapid brain development of adolescence.
It says the “use of puberty blocking medication typically occurs for several years, and provides an opportunity to learn how the teenage brain develops in the absence of sex hormones”.
In 2015, Dr Telfer was quoted in the men’s magazine GQ Australia explaining medical interventions.
“At [puberty] we can start someone on puberty blockers,” Dr Telfer is reported as saying. “They don’t stop growth generally, or your brain from maturing emotionally and cognitively, they just stop the sexual characteristics from developing.”
In 2018, Dr Pang was among the authors of an article billed as “the first systematic review” of hormonal treatment for trans youth.
It reports only “low-quality evidence” that puberty blockers and opposite-sex hormones do what they are supposed to do physically, while evidence on their “psychosocial and cognitive impact [is] generally lacking”.
A missing study
Apart from the international evidence reviews by NICE, Cass review documents make multiple references to learning from clinical practice both within and beyond the UK.
As for the US-centric guidelines said to be underplayed by the Cass review, both the Endocrine Society and WPATH documents feature in the first reference of the Cass report — the landmark 2015 Dutch “empirical ethical study” of the dilemmas posed by puberty blockers. [Clarification: the Endocrine Society document is the earlier 2009 version of the Hembree at al guideline.]
With the prominent Dutch clinician Dr Peggy Cohen-Kettenis among its authors, this study makes the point that despite the Endocrine Society and WPATH advising early use of puberty blockers for gender dysphoria, “in actual practice, no consensus exists” for this practice.
The paper identifies seven fundamental points of clinical disagreement, including the capacity of children to consent to puberty blockade and the psychological effects of this intervention.
The study reached its conclusions following interviews and surveys of 17 treatment teams with 36 health professionals across 10 countries in North America and Europe.
Far from proving international consensus, the Endocrine Society and WPATH guidelines were “strikingly” regarded by various clinical teams as both “too liberal and too conservative”.
Clinicians were deeply divided on philosophical, ethical and clinical issues.
(The Cass review also notes a troubling “lack of open discussion” about fundamental issues to do with youth gender dysphoria; nervousness on the part of frontline health professionals; and the “toxicity” of the wider social debate.)
One psychologist quoted in the 2015 Dutch empirical ethical paper says: “I have met gay women … who would certainly have been diagnosed gender dysphoric as children but who, throughout adolescence, came to accept themselves. This might not have happened on puberty blockers”.
The paper notes that “more and more treatment teams embrace the Dutch protocol [of medical transition starting with puberty blockers] but with a feeling of unease.
“The professionals recognise the distress of gender dysphoric youth and feel the urge to treat them [yet] most of these professionals also have doubts because of the lack of long-term physical and psychological outcomes.
“The possible consequences of suppressing puberty for cognitive and brain development are unclear and debated at this moment.”
The paper concludes there can be “no true consensus on treatment” without long-term research involving multiple clinics around the world.
This 2015 Dutch empirical ethical paper is not cited by the policy statements from the American Academy of Pediatrics or the Endocrine Society, nor by the guideline of the Royal Children’s Hospital Melbourne.
Asked by GCN if there is more or less consensus today, the leading Dutch clinician Dr de Vries said “it would be of interest” to repeat the 2015 study.
What about the brain?
A reading of the interim Cass report suggests that the full extent of uncertainty about puberty blockade is still unfolding, with a sharper focus on the unknown effects on cognitive development when natural sex hormones are suppressed by these drugs.
“It is known that adolescence is a period of significant changes in brain structure, function and connectivity,” the report says.
“Animal research suggests that this development is partially driven by the [natural] pubertal sex hormones, but it is unclear whether the same is true in humans.
“If pubertal sex hormones are essential to these brain maturation processes, this raises a secondary question of whether there is a critical time window for the processes to take place, or whether catch up is possible when [cross-sex] oestrogen or testosterone is introduced later.”
The report cites an ambitious project whereby 24 international experts in fields including neurodevelopment and adolescence collaborated to identify the key research questions to elucidate the effects of puberty blocking on cognition and the brain.
The 2020 “Consensus parameter” paper, with American psychologist Dr Diane Chen as lead author, drew on experts from the US, Europe and Scandinavia.
“The pubertal and adolescent period is associated with profound neurodevelopment, including trajectories of increasing capacities for abstraction and logical thinking, integrative thinking (for example, consideration of multiple perspectives), and social thinking and competence,” the paper says.
“The combination of animal neurobehavioural research and human behaviour studies supports the notion that puberty may be a sensitive period for brain organisation: that is, a limited phase when developing neural connections are uniquely shaped by hormonal and experiential factors, with potentially lifelong consequences for cognitive and emotional health.”
The Consensus paper recommends complex longitudinal research involving multiple gender clinics and more than one comparison group (including untreated trans youth) in order to get a big enough sample and to isolate the outcomes caused by puberty blockers.
GCN put questions to the Cass review, Royal Children’s Hospital Melbourne, Dr Telfer, Dr Pang and the Murdoch Children’s Research Institute. In a rare public comment in December 2019, RCH issued an open letter saying its treatment guideline was “peer reviewed at the highest level”, and the gender clinic relied on “the best available medical evidence” and followed “strict clinical governance standards”.
Thanks Bernard - you really do put a lot of work into this.