
'Stop this now, Minister'
Once famous for caution, the Amsterdam gender clinic stands accused of undermining its own safeguards


The gist
The Netherlands’ Health Minister Dr Ernst Kuipers has a duty to take action to protect autistic minors from medicalised gender change at the famous Amsterdam clinic, according to the Dutch opposition politician and physician Dr Nicki Pouw-Verweij.
“I think the minister should immediately put his foot down and say, ‘[Transitioning autistic minors is] not something we’re going to do’,” Dr Pouw-Verweij told GCN.
“We see all these girls with autism showing up [at gender clinics], and we don’t know why. So, don’t treat them [medically] until we know.”
Dr Pouw-Verweij, a representative of the liberal-conservative party Right Answer (JA21), was commenting on a recent paper from liaison psychiatry doctor Karl Gerritse and other researchers at the Amsterdam gender centre detailing “clinical challenges” with adolescent and adult patients.
The September 2022 Gerritse paper—with a leading Dutch clinician, psychiatrist Dr Annelou de Vries, among its authors—declares that autism and psychiatric disorders such as schizophrenia should not automatically stand in the way of gender transition with hormonal and surgical interventions. (Note: an earlier version of this article stated incorrectly that Dr Thomas Steensma was an author.)
The Gerritse study revolves around the case of “Emma”, a biological male diagnosed at age 8 with autism spectrum disorder, who “barely spoke” and sent her surprised parents a text message with the single word “transgender” when she was 16.
At first, Emma’s parents thought her wish for trans treatment might be “a temporary obsession”, and the treating psychiatrist was concerned she had unrealistic expectations of this treatment. After a trial of testosterone suppression and her agreement to have psychomotor therapy, Emma was started on the cross-sex hormone oestrogen.
The authors of the Gerritse paper conclude it is “unethical” to impose a blanket ban on medical transition for patients with “psychiatric problems [in addition to gender dysphoria] and/or impaired competence.”
The Amsterdam clinic, which pioneered the use of puberty blockers to interrupt natural but unwanted sexual development, is often said to be more cautious in selecting patients than centres internationally that follow the radical American “gender-affirming” treatment approach.
For the landmark Amsterdam studies leading to key papers in the 2010s, patients had to have the distressing condition of gender dysphoria stretching back to early childhood—most were natal males—and to be free of psychological disorders that would interfere with diagnosis or treatment.
The reason for strict eligibility rules was to vouchsafe an enduring transgender identity, while minimising “false positives” and regret after irreversible medical treatment.

The Gerritse paper, one of several signs of a more permissive approach to treatment at the Amsterdam clinic, concedes there is no evidence on treatment outcomes for autistic patients who transition. It notes that what looks like feelings of gender conflict may actually be symptoms of psychosis or autism.
The paper also acknowledges the difficulty for young patients with autism to understand the consequences of life-altering trans interventions, such as sterilisation and the lost chance to have their own children.
But the researchers emphasise the “depathologising” and “emancipation” of trans and non-binary identities, the “highly evolving” social discourse on gender diversity, and the need to reduce “stigma” while enabling “treatment access”.
They use the newer, less pathological term “gender incongruence”, rather than gender dysphoria, which required “clinically significant distress” for diagnosis and invasive medical treatment. Gender incongruence is seen as a better fit with ideas of patient autonomy and self-determination.
“I'm not the one who decides whether people go on for medical treatment. That is really a joint process between the client and the healthcare provider. We don’t see ourselves as gatekeepers but rather are focused on customisation. There are people who need very little counselling and have realistic expectations, but there are also people who report needing more care” — clinical psychologist Dr Thomas Steensma, Amsterdam gender clinic, reported by Nederlands Dagblad, 9 September 2022
Another pillar of the Dutch protocol—restricting hormonal and surgical interventions to cases of persistent childhood-onset dysphoria—was discontinued in the 2018 Netherlands quality standard for trans medical treatment.
This quality standard, currently under review, should look into curtailing the psychiatric evaluation required before medicalised gender change, according to a 2021 motion passed by the Dutch parliament in depathologising mode.
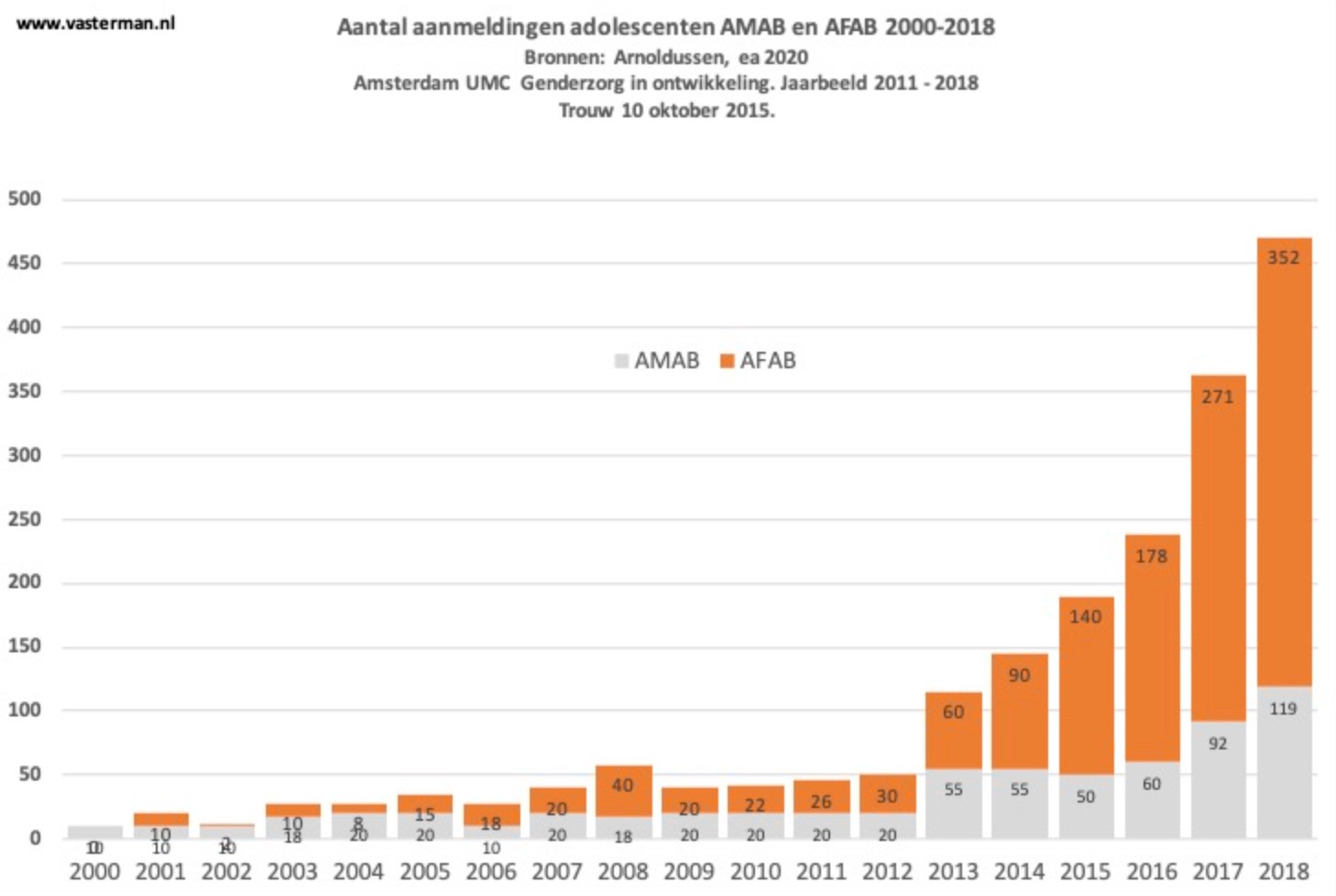
Applications for gender clinic care by Dutch minors have risen from 883 in December 2018 to 2,500 in January 2022, according to Health Minister Kuipers. At the Amsterdam clinic last year, there were 2,772 young people on the waiting list.
Chart: Adolescent patient registrations at the Amsterdam gender clinic, with the orange column showing the number of biological females. Source: Dr Peter Vasterman
‘Defend the doctors!’
Dr Pouw-Verweij, whose medical training a decade ago exposed her to the rationale of the Amsterdam gender centre, said clinicians had recently told her in confidence that its once cautious culture had changed, and that they found themselves struggling to insulate sound clinical decisions from the pressure of trans rights activists.
She said Health Minister Kuipers (who trained as a gastroenterologist) should come to the defence of these cautious doctors by putting on hold medical treatment of minors.
This would create a breathing space for critical inquiry into the reasons for the unexpected shift in patient profile from the classic mostly male, early-onset gender dysphoria to today’s surge of mostly female adolescent-onset cases.
“Where are these girls coming from? Is there a big social element, are they even actually transgender?”, Dr Pouw-Verweij said.
“Do they experience gender dysphoria? Or are there other things going on? We’re also seeing a lot of co-morbidities — for instance, autism.”
On the podcast Gender: A Wider Lens last month, Jan Kuitenbrouwer—one of the few Dutch journalists to break the taboo on critical coverage of youth gender medicine—said the Amsterdam clinicians were in an unenviable position.
“They’ve been doing this [paediatric transition] for 30 years and now, all of a sudden, there’s all this scrutiny,” he said.
“I think, with themselves, it’s slowly sinking in—‘My god, what have we done? We have corrupted this protocol step-by-step.’ There’s going to be a moment when they’re going to have to own up to all this.”
Video: The documentary Dead Name is an example of the growing pushback to the American gender-affirming treatment model
The detail
Dr Jilles Smids, a philosopher at the Erasmus University Medical Centre in Rotterdam, said he thought the Amsterdam clinic had misconstrued patient autonomy.
“In healthcare, autonomy never means the right to receive the treatment the patient wishes for,” he told GCN.
“Autonomy is first and foremost a right to give informed consent to treatments that are indicated, on the basis of a proper differential diagnosis.
‘What’s more, without sufficient self-understanding, there can never be an autonomous choice for medical transition.
“If the trans adolescent would be open to it, exploration with a good psychologist could facilitate such understanding.”
He noted statements by Dutch gender clinicians that they are not “gatekeepers.”
“But given that a diagnosis of gender incongruence is a requirement and given the fact that co-occurring psychological problems often cloud the picture, it’s simply their professional duty to slow down and just say ‘no’ to those who would be harmed by medical transition,” Dr Smids said.
He also challenged the statement in the 2022 Gerritse paper that there is “extensive evidence” for the effectiveness of trans medical treatment. The systematic review cited in the paper (Murad et al, 2010) concludes there is only “very low quality evidence” of benefits.
“[The Amsterdam clinicians] should have grounded confidence that their treatment, on balance, benefits adolescents—such evidence is, unfortunately, lacking,” Dr Smids said.
“So, I think it is very important that the Netherlands change course and follow the recent cautious and much more sensible approach of Finland and Sweden.”
Gender-affirming pressure
Media sociologist Dr Peter Vasterman—a retired academic who co-wrote with Jan Kuitenbrouwer an opinion article last December calling for a “critical, independent evaluation” of gender medicine in the Netherlands before any expansion of capacity—said the Dutch model did seem to offer more psychological assessment than the American gender-affirming approach.
“Nevertheless, what the patient wants is still leading in this whole process,” Dr Vasterman told GCN.
And there was “anecdotal proof” that sometimes patients were getting access to medical treatment after only a very short talk with a psychologist.
Dr Vasterman said that if the Netherlands enacted a law against “conversion therapy” involving not only sexual orientation but self-declared gender identity, this would “reinforce” the local influence of the gender-affirming model, thereby “chilling” the more exploratory psychotherapeutic approach.
Bans on conversion therapy are often targeted at churches, but Christian influence may help explain the approach to treatment at the Amsterdam clinic, part of the city’s Free University (VU), which was founded as a Protestant Christian institution in 1880.
“I think the whole attitude of the VU [gender clinicians] is drenched with the idea of compassion, to relieve suffering [despite lack of good evidence for the efficacy of treatment],” Dr Vasterman said.
“Now, as critical studies pile up, they still cling to the idea that medical treatment is necessary to relieve suffering—despite the fact that distress have been removed from the gender incongruence criteria.
“For more than two decades [the Dutch clinicians] represented the progressive and humane treatment for these [trans-identifying] children, [treatment] that became a huge international success. It is difficult to step down from this glamorous pedestal.”
Media coverage of gender clinics often has an evangelical tone.
“The media and the audience are fascinated by these young people going through such a radical transition,” Dr Vasterman said.
“They are presented as heroes who—despite prejudice and difficult medical procedures—try to ‘become who they are.’
“Because these young people are also sort of victims—of being ‘born in the wrong body’—critical questions are never asked, it’s all about how they and their parents and friends cope with the gender transition” — Dr Peter Vasterman
“The physicians are part of this, they help these young people, so they [supposedly] do not need to be scrutinised.
“Asking difficult questions is almost disrespectful: how dare you doubt this? Also important is the visual aspect of the transition, that makes it very attractive for television.”
Even so, a more lively than expected debate has begun in the Netherlands following a radical draft law for legal gender change at home, and news from abroad of detransitioner Keira Bell’s 2020-21 litigation against England’s Tavistock gender clinic.
The Dutch gender self-identification proposal has generated some serious pushback in the parliament, and not only from Christian and conservative politicians.
“Up until recently, nobody would dare criticise trans care in the Netherlands,” said Dr Pouw-Verweij. “We are a liberal country proud of our open-mindedness and inclusion, so diverting from that norm could have big implications both professionally and personally.”
What we don’t know
In the city of Nijmegen, Radboud University’s Centre of Expertise in Sex & Gender has injected a dose of caution into the debate.
“The group of young children who say they have gender problems has grown so large that it raises the question of whether all of these children also need medical care,” Dr Chris Verhaak, a researcher and clinical psychologist at the centre, told the current affairs program EenVandaag.
“Are they all best served by hormone treatments or gender-specialised psychotherapy?
“There is still a lot that is unclear with these children. What is the effect of peer pressure, of images in the media and of other problems at play, such as autism or a traumatic event or problems in the family?
“It’s wonderful that the transgender [treatment] pathway is there, but everything that is there to prevent medical intervention, you have to use.
“Puberty hormones normally set off psychosexual development. So if you inhibit those [with puberty blocker drugs], then the children hardly have that development. I think that’s a big concern. What does that mean for those children and adolescents, and what does that mean for sexual development later in life?”
Anything but bio sex
Dr Pouw-Verweij has tried to draw attention to the overlooked clinical implications of making it easy for minors to change legal gender.
At age 16, an expert opinion of enduring opposite-sex identity will no longer be needed, and official gender change will be possible for children under 16 with an application to the court.
“If people [including minors] can change their gender or their sex in their passport with basically a snap of their fingers, how are doctors going to tell them that they can’t medically alter their sex as well?”, Dr Pouw-Verweij said.
She is likely to find support for her concerns in the populist politician Caroline van der Plas, whose farmers’ protest party (BBB) looks like being a force to reckon with in the upper house of parliament following the March 15 provincial elections.
“I am afraid that this [self-ID gender] law will cause children to make decisions that they are not yet ready for, that it is made too easy and they will regret it later. Everyone should be able to live the way they want, but a process like this has to be done very carefully” — Caroline van der Plas, Nederlands Dagblad, 18 March 2023
Dr Pouw-Verweij said the exponential increase in teenage females seeking medicalised gender change could not be explained simply by greater social acceptance of trans or non-binary identities.
“There has to be a social element. If you look at TikTok or Instagram, there’s a very big movement going on there that preaches self-acceptance, but also preaches that, for instance, it is a great idea for females to have a double mastectomy, to embrace your inner non-binary identity or your male identity.
“And [this movement] is just very focused on not accepting your boring [biological] sex.”
Dutch detransition
Maarten, age 23, had identified as female and began transition at 16. Now he regrets treatment with cross-sex hormones and facial feminisation surgery. “Self-acceptance was never discussed with me. Going into transition was the stupidest thing I could have done. It turned out not to be the solution to my problems at all. It only made me feel worse. Before my transition I had never seriously considered suicide, but after that I was really afraid I would attempt it. I was living on the fourth floor, but luckily there is such a thing as the suicide-prevention line.”
Source: HP/De Tijd, 31 October 2022
Iris, age 22, was 15 and depressed when she first came to the gender clinic. She took puberty blockers and synthetic testosterone, and had a double mastectomy. She says the clinic operated like a funnel. “Everything leads to the diagnosis of gender dysphoria. I had a trauma from my back surgery; I was depressed with symptoms of anxiety. I did not feel comfortable in my body and was confused about my sexuality. It was hard to talk to my parents, and I suffered social anxiety. All those symptoms were labelled as transgender problems.” She lived five unhappy years as a trans man. “I didn’t feel at ease with men or women.” Now she recognises herself as a lesbian. “I would have liked to know [when I was 15] that it is also okay to be a boyish girl and that being a lesbian does not mean you cannot be a woman.”
Source: de Volksrant newspaper, 24 February 2023
‘Not good enough’
Dr Pouw-Verweij is one of the politicians who has put formal questions to Health Minister Kuipers seeking to understand the local implications of the intensifying international debate over the Tavistock clinic and the dogmatic gender-affirming treatment model.
She said: “I wasn’t very satisfied with his answers. Basically, he said—‘We have the best [gender clinic] system in the world, we’re doing fine. We’re not doing gender affirmation. And self-ID law is not related to medical transition.’
In response to those questions, Dr Kuipers insisted that Dutch clinics carry out “comprehensive assessment [including] all aspects of the psychosocial and sexual development of the child/young person—for example, other possible [non-gender] causes of psychological suffering are also considered.”
He said it was not his role as minister to interfere in decisions about gender treatment.
Dr Pouw-Verweij said nobody was asking him to intervene in the privacy of the doctor-patient relationship.
But she said the government, which is run by a centre-left coalition, should certainly get involved in the public health questions raised by the unprecedented international surge in troubled teenage girls seeking gender medicine.
The more permissive “radical inclusion” approach to gender medicine implied that denial of these interventions was a denial of someone’s right to live an authentic life, she said.
“But if you’re looking at it from a medical standpoint, which I think we should, then you have to ask, what is the clinical problem here?
“And what is the treatment that has the highest chance of doing the most benefit and doing the least harm?
“And if somebody is also autistic, and you can’t reasonably exclude the possibility that the autism, combined with puberty symptoms, is causing secondary gender dysphoria, well, then the risk of harm is so big.
“You should decide not to treat this person until you’re definitely sure that it’s primary gender dysphoria.”
Psychotherapy would be a safe treatment approach, but “not puberty blockers or hormones, let alone actual surgery,” Dr Pouw-Verweij said.
“[But] now there’s this mindset that if you question somebody’s transgender identity, then you’re a transphobe-bigot. And so even for psychologists who are supposed to [apply] safeguards, it’s really hard to ask [therapeutic] questions—because an actual mob will show up at the hospital [protesting with signs].”
In June 2021, below the headline “Transgender care under fire: ‘A psychologist has the power to decide over your body’”, the Dutch newspaper NRC reported protests demanding easier, quicker access to gender medicine.
One protestor, Noah from Leiden, said: “I have friends who are autistic and therefore have to put more effort into proving they want to transition.” Another protestor held a sign saying “Not Trans Enough? VUck off!” (VU is the university that is home to the Amsterdam clinic) and this person told the journalist, “Your own identity is what you know best.”
But Dr Pouw-Verweij believes the judgment of history may take a different view.
“I think that we are going to look back on this and realise there were a lot of vulnerable, confused girls that received puberty blockers, testosterone, mastectomies, all of these things with long-term consequences.
“And [we will realise these patients] never experienced any primary gender dysphoria, and therefore, we were not effectively treating anything. So, there was no benefit and only harm.
“And so, of course, [Health Minister Kuipers] should at least put a halt to [this medicalisation] until we know what we’re looking at and how we should effectively treat it.”
Note: GCN put questions to the Amsterdam clinic and Health Minister Kuipers
Wow, what a great and extensive update on the Dutch situation. Thank you, Bernard!
I would be careful with calling the BBB party 'populist', btw. This is often done to right wing parties that the left or the ruling parties don't want to have to deal with. It's a highly subjective qualification but also, it doesn't paint BBB in a fair light because it's a party that - despite rhetoric that you can disagree with (like I do often) - seems to so far have a constructive attitude; it's fair opposition in a parliamentary democracy.
There also seems to be a translation mistake, I think? (I'm Dutch so I could be wrong) Pouw-Verweij is quoted as saying 'transphobe bigot'; shouldn't that be 'transphobic bigot'?