
Gay history hijacked
Plus: Canada breakout; hypocrisy in France; Swedish data puzzle; judicial pronouns; captured health regulator in Oz; doublespeak from the American Psychological Association; new Chilean detrans book


GCN global briefs
Hidden agenda
United Kingdom | The UK government’s promise of a “trans-inclusive” ban on unethical conversion therapy is misleading, according to the LGB Alliance. In its latest policy bulletin aimed at MPs, the alliance says: “Any act that might be considered a conversion practice is already illegal. The sole purpose of new legislation would be to ensure that therapists, and other professionals working with children, automatically affirm every child who says they are trans. The abhorrent, historical abuses suffered by gay people are being used by trans lobbyists to convince the public that this legislation is needed”.
In The Spectator magazine, writer Lionel Shriver argues that the real conversion therapy of our times is “the industry of ‘gender transition’ itself”. She has her own candidates for prohibition. “Make it illegal to pretend to ‘transition’ minors who may be disturbed mentally but have nothing physically wrong with them. Prohibit scientifically illiterate teachers and counsellors from inculcating children with the idea that sex is anything other than permanent and that there are any more sexes than two.”
And Shriver welcomes the recent decision of the US Supreme Court striking down Colorado’s anti-conversion therapy law as an unconstitutional fetter on free speech. She writes: “Capable of affecting similar conversion therapy bans in 21 other states, the decision was 8-1, endorsed by two liberal Democratic appointees. (Baffled by the definition of the word ‘woman’, the single dissenting justice is an idiot.) The majority sensibly characterised talk therapy—speech—as speech, not merely professional ‘conduct’. They also objected to the asymmetry of a law that prohibits questioning patients’ conviction that they were supposedly born in the wrong body, but doesn’t apply to therapists who eagerly ‘affirm’ the delusion. This constitutes state discrimination based on viewpoint—aka wokey authoritarianism”.
Speaking up
Canada | A prominent Canadian gender clinician, Karine Khatchadourian, has gone public with her shift to a more cautious stance on gender medicalisation. This is big news in a country where gender ideology is strong. Dr Khatchadourian’s interview with journalist Sharon Kirkey made the front page of the National Post, with the caption: “She was one of the first doctors in Canada to provide hormones to trans-identifying youth. She now believes most children should not be medicalised”. She does not reject the gender-affirming model. However, Kirkey reports, “Khatchadourian favours aligning with Sweden and Finland’s approach, where puberty blockers and cross-sex hormones are reserved for children and teens with a history of gender dysphoria that started in early childhood and has persisted for many years”.
The dominant patient profile in today’s gender clinics is teenage females with no early childhood dysphoria; the influence of social media and peer groups is a suspected factor in the unprecedented growth of this profile since the 2010s.
Other Canadian gender clinicians have privately shared similar concerns about paediatric gender medicine without “detailed and lengthy assessments”, according to the physician and academic Dr Laura Targownik, who is trans and blogs as The Data-Driven Transsexual. Danielle Smith, the United Conservative premier of the province of Alberta, has hailed Dr Khatchadourian’s rethink as a sign that “A major shift is underway”. In February 2024, Ms Smith foreshadowed Canada’s first restrictions on access to puberty blockers, cross-sex hormones and gender surgery for minors. That Alberta policy is now in operation and potentially a model for other, more Left-leaning provinces, as Dr Targownik writes.
Meanwhile, in Quebec, a teacher who refuses to lie to parents about the covert social transition of a child at school, has launched a court challenge under Canada’s Charter of Rights and Freedoms.
“I could not live with myself if I did [lie, as required by school policy],” the teacher says. “I will not look [parents] in the eye and intentionally lie about the fact that we are enabling their child to undergo a significant psychosocial intervention without their knowledge. Transparent collaboration with parents is essential to my role as a teacher and is critical for the long-term wellbeing of children. Lying to parents about how we are treating their children, or about what is going on with their children at school, violates the principles of my vocation”. The order to lie also violates the teacher’s freedom of expression and conscience under the Charter, according to her lawyer.
François Chapleau, emeritus professor of biology at the University of Ottawa, has set out the obstacles faced by parents in the gender ideological milieu of Quebec. “[In the sex-education curriculum] children are taught, from a very young age, a pseudoscientific notion of identity detached from the reality of the body and biological sex, as if the words ‘boy’ and ‘girl’ were merely arbitrary labels ‘assigned’ at birth, unrelated to chromosomes or genitalia,” Professor Chapleau writes.
Boys on blockers
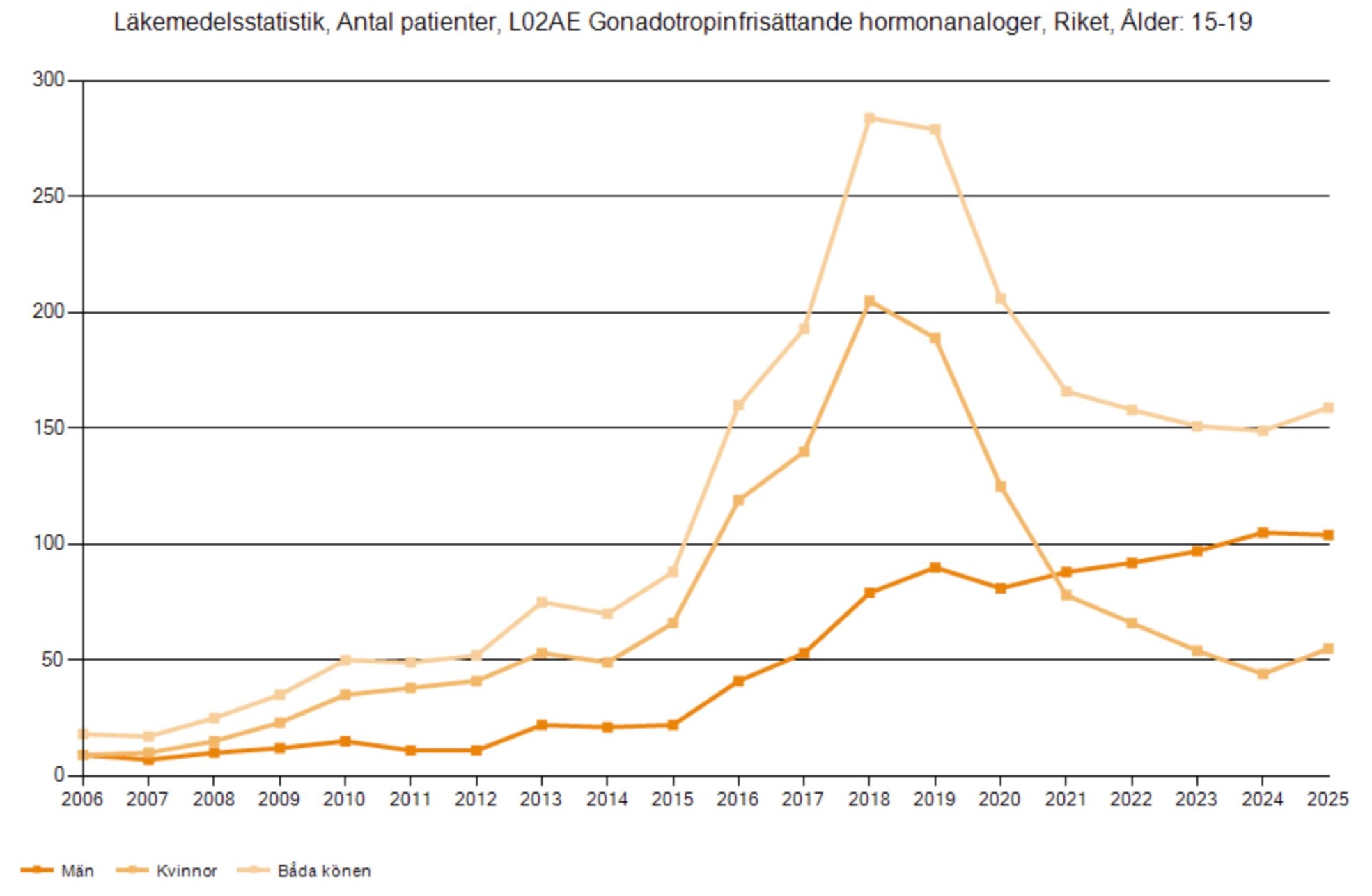
Sweden | Despite Sweden’s adoption of a more cautious treatment policy in 2022, the number of male teenagers on puberty blockers has increased. For both males and females aged 15-19, puberty blocker use peaked in 2018-2019. Since then, prescriptions of blockers for females fell sharply, albeit with a rise in 2025. The number of males on blockers showed a steady increase from 2020-2024 before levelling off in 2025. The number of puberty-suppressed males in 2025 was about 50 more than the number of females; at peak usage, females had outnumbered males by more than 100.
Paediatrician Mats Reimer, who extracted the figures from an open database, says that “some clinics in Sweden do not appear to be following the cautious treatment policy, though this applied to those under 18”; his data includes 19-year-olds. Dr Reimer told GCN he believes “the healthcare system should delay hormone treatment for gender dysphoria until after the age of 25”. He was unsure why males were now over-represented, “but I’d guess it’s because male puberty makes it harder to later ‘pass’ as the opposite sex”. It could also be that clinicians believe the evidence base is less weak for males with an early childhood history of dysphoria.
Puzzle: Males overtake females in puberty blocker usage nationally in Sweden
Two-faced
America | The American Psychological Association (APA) has been accused of straddling two contradictory positions on youth gender dysphoria. Kurt Miceli of the watchdog group Do No Harm makes this claim in an April 20 letter to the Federal Trade Commission (FTC), which has been investigating unfair or deceptive practices in paediatric gender medicine.
Dr Miceli says the commission should take a close look at the APA. In 2024, he says, the APA adopted “a strong ideological” stance in favour of gender-affirming interventions. A year later, however, the APA issued a more cautious statement stressing that a diagnosis of gender dysphoria “is not an automatic or singular pathway to medical intervention or even social transitioning”. The APA insists these two positions are consistent.
Dr Miceli says: “The APA cannot have it both ways. These conflicting messages, which will influence how psychologists and other providers counsel children and families on irreversible medication interventions, are misleading to consumers, patients, and the FTC”.
Return to common sense: Dr Miceli of Do No Harm says minors confused about gender need psychological support, not a hurried medical pathway
Attack of nerves
France | The prestigious Collège de France, an institution of higher education which trumpets its role in the free dissemination of cutting-edge research and ideas, has de-platformed a conference that features a talk on detransitioners.
The conference—Children as the target of ideologies—was booked for June 22 this year and organised by the French group The Little Mermaid directed by clinical psychologist Dr Céline Masson and child psychiatrist Dr Caroline Eliacheff. Prominent critics of paediatric gender medicine, these two health professionals were to discuss detransition with psychotherapist Stella O’Malley, Genspect’s founder, at the Collège de France. But the conference has been moved and delayed, not cancelled. It is expected to go ahead in October, with the French Senate as its venue and Senator Jacqueline Eustache-Brinio of the Republicans party as its patron.
Youth gender dysphoria is just one of several broader themes at the conference to do with well-intentioned but harmful interventions with children. The conference flyer says: “Virtuous, socially acceptable hatred [of children] is an ideologised perversion that legitimises educational, psychological or medical practices which deny the needs, psychological development and specific status of the child, a person in the making. In the name of certain values—such as tolerance, progress, inclusion and the fight against discrimination—we are manufacturing a child, a product of adult fantasies”.
The French politician and High Commissioner for Childhood, Sarah El Haïry, was to sponsor the June 22 conference at the Collège de France but withdrew, citing reservations about The Little Mermaid group, which is often smeared as “transphobic”. And then, on April 13, the Collège de France retracted its offer to host the conference, claiming the event would undermine its “principle of neutrality” and risked causing “confusion regarding responsibility for its content”.
In the media outlet Le Point, one of the conference presenters, Sylvie Tordjman, a prominent professor of child and adolescent psychiatry, wrote that in seeking to protect itself from criticism, the Collège de France had contributed “precisely to the phenomenon it claims to avoid: the absence of debate”.
His Honour’s pronouns
America | US District Court judge Mustafa T Kasubhai has ruled unlawful a 2025 declaration by Secretary of Health and Human Services (HHS) Robert F Kennedy Jr that hospitals offering “sex-rejecting procedures” to minors could lose funding under the Medicaid and Medicare programs. The 12-page Kennedy declaration notes the findings of the HHS Gender Dysphoria Report and international inquiries leading to the view that gender medicine for minors is neither effective nor safe.
In his ruling Judge Kasubhai says the peremptory nature of Mr Kennedy’s intervention “caused chaos and terror”. The judge, appointed by the Biden Democratic administration, signed his decision with (he/him) pronouns.
Gender jargon
Europe | The European Court of Justice has found Hungary breached EU law with measures presented by the member state as essential for child protection and the right of parents to raise children according to their own values. In a video summary, the court’s president, Koen Lenaerts, contends that EU law does not allow a “stigmatising” ban on the development or distribution of content portraying or promoting, as he puts it, “divergence from the personal identity corresponding to the sex assigned at birth, sex reassignment or homosexuality”. He says Hungary’s amendments infringe on the “rights of non-cisgender or non-heterosexual persons”. This, he claims, runs counter to the pluralistic foundation of the EU.
Improbable protocol
The Netherlands | A retrospective study at the Amsterdam clinic, home to the puberty blocker-driven “Dutch protocol”, reveals “a fundamental incoherence” in approach, according to an analysis by Hermes Postma published by Genspect. The study involved 1,470 patients given a first assessment between 2009 and 2019; 264 of these did not proceed to puberty blockers or cross-sex hormones. Postma notices a shift in the rationale for puberty blockers, which used to be justified as affording a child “time to think” and explore gender. Now, the Dutch researchers instead ask “whether adolescence is the right timing”, while recording the fact that many who went through natural puberty nonetheless sought treatment later.
“The same medication used without a formal diagnosis to create an exploratory space is elsewhere described as medically necessary care within the basic health-insurance package,” Postma writes. “This circular logic—natural puberty gives space, blocked puberty gives space, and blockers are also given when no diagnosis exists—reveals a fundamental incoherence at the heart of the protocol’s rationale.”
Meanwhile, in the Dutch magazine HP/De Tijd, columnist Jan Kuitenbrouwer hails the latest study from Finland—which shows a dramatic increase in the need for specialised psychiatric help after medical transition—as “another nail in the coffin of the Dutch protocol”.
Nordic imperative
Finland | The Finnish paper—“Psychiatric Morbidity Among Adolescents and Young Adults Who Contacted Specialised Gender Identity Services in Finland in 1996–2019: A Register Study”—is still generating (patchy) media coverage. In combative mode, the editorial board of The Wall Street Journal says: “Remember the ‘follow the science’ mantra? Finnish researchers have done so in a comprehensive new report on the mental-health outcomes for youth who undergo gender reassignment treatment. The results are a rebuke to those who call for irreversible interventions for children”.
The Finns made use of the country’s healthcare register to guarantee inclusion of all former patients, as well as a large group of matched controls. “This is a study with proper control, and non-selective participation, so rare, so beautiful, almost like a unicorn,” tweeted researcher Ray Yuan Zhang of the Evidence Bridge. In The Australian newspaper, columnist Claire Lehmann welcomed the unusually rigorous longitudinal study from Finland, and concludes that, “In 2026 we have enough evidence to know that rushing kids into a medicalised gender transition is unwise and unsafe”. The Swiss German-language paper, Neue Zürcher Zeitung devoted a full page to the Finnish study with the headline “A gender change does not make trans adolescents happier”.
On his Substack, journalist Benjamin Ryan put trans activist critiques of the study to one of its authors, adolescent psychiatrist Riittakerttu Kaltiala, who responds in some detail. In a webinar hosted by Australia’s National Association of Practising Psychiatrists, Professor Kaltiala addresses some of the misconceptions about the study at the 38-minute mark. She also highlights the unacceptable level of “personal defamation and threats against researchers” in the field of youth gender dysphoria (from the 55m mark). Professor Kaltiala took questions from the 57:30m mark. The recorded webinar is freely available until May 4.
Origin stories: Psychiatrist Dr Stephen Levine, a veteran in the field of gender dysphoria, teases out the links between adolescence and identity
In print
Chile | Nicolás Raveau, a Chilean detransitioner who used to be a trans activist, has published a book titled “No Longer Trans: Insights from within the LGBT activist movement and its institutional decline”. Apart from his personal odyssey, Raveau traverses the policy landscape, including Chile’s Program of Support for Gender Identity (Programa de Acompañamiento a la Identidad de Género, PAIG), which was promoted as an uncontentious psychosocial intervention. Yet, as Raveau writes, “the PAIG facilitates an accelerated and premature social transition from the age of three. What is more serious, however, is that it leads directly to hormone treatment from the age of ten and provides a ‘range’ of surgical procedures for the future”.
Ideological capture
Australia | The Australian Health Practitioner Regulation Agency (AHPRA), which has silenced a psychiatrist critical of the gender medicalisation of children, has a conflict of interest as a paid-up customer of the trans activist lobby ACON, according to The Australian newspaper. “Documents released under [Freedom of Information law] reveal howAHPRA developed an LGBTIQA+ strategy based on adherence to the gender ideology of ACON, extending to the way it regulates health practitioners,” journalist Stephen Rice reports.
“In correspondence obtained by The Australian, AHPRA boss Justin Untersteiner states that the regulator’s engagement with ACON and accreditation group Rainbow Health Australia guides ‘the way we regulate and fulfil our purpose of ensuring the preservation of public safety’. The revelations follow claims Australia’s medical complaints system has been weaponised by gender activists using a compliant regulator to intimidate psychiatrists who speak out against gender-affirming treatment such as puberty blockers, while shielding doctors who promote them.”
Blind to the evidence
America | In the northern winter just gone, “Mehmet Oz, the head of the Centers for Medicare and Medicaid Services, summoned the leaders of the country’s major medical societies to his office for what he called a ‘grand rounds’—a hospital term for a meeting where doctors discuss complex cases,” journalist Jeremy Peters reports in The New York Times.
“The topic was one of the most contentious in American medicine: Transgender medical care for teenagers. Dr Oz pressed on a question that hangs over the entire field: Why did these organizations recommend medical intervention for young patients—including hormone treatment, puberty blockers and surgery—when the research on whether it helped young patients in the long term, especially on mental health, was inconclusive?” Most of the societies defended their gender-affirming positions, but Dr Oz highlighted the independent evidence reviews in the UK, Finland, Sweden and New Zealand leading to policies restricting hormonal treatment of minors.
Tweaking the trial
United Kingdom | The UK “PATHWAYS” puberty blocker trial should incorporate safeguards based on adverse effects documented when the same hormone suppression drugs are used with gynaecological conditions such as endometriosis, uterine fibroids, and polycystic ovary syndrome, according to a recent journal article. The author, Canadian research scientist Sarah CJ Jorgensen, also argues that the PATHWAYS trial’s proposed use of a wait-listed control group could distort results via expectancy and nocebo (or negative placebo) effects.
The paper was finalised before the trial was put on hold in February, with renewed ethical concerns. One possible change in eligibility for the research is a minimum age of 14, meaning later in puberty than with the original design.
“If PATHWAYS changes the inclusion criteria to 14-16 years, then I think the risk-mitigation strategies I discuss in my commentary would apply to a larger proportion of the enrolled females, since most will have reached later stages of puberty (unless they specifically select for females with delayed puberty),” Dr Jorgensen told GCN. “My concerns about nocebo and expectancy effects would still be relevant if they use a wait-list control, though as I note in my commentary, using established forms of menstrual suppression as a blinded comparator in post-menarcheal females [those who have experienced the onset of menstruation] would largely avoid such effects.”
Tongue-tied
America | There has been claim and counterclaim since The New York Times reported in February that the American Medical Association (AMA) had agreed with the new, cautious policy on paediatric gender surgery adopted by the American Society of Plastic Surgeons (ASPS). “For the first time, two major medical groups have backed limitations on gender-related surgical treatments for minors in the US,” The Times reported, citing an AMA statement that, “In the absence of clear evidence, the AMA agrees with ASPS that surgical interventions in minors should be generally deferred to adulthood”. In March, the AMA’s board chair disowned the statement amid claims that it contradicted existing policy. The Times stood by its report, producing the full statement given by the AMA’s chief communications officer.
“The ongoing controversy at the AMA over what exactly their position is demonstrates how divided the medical field has become over this issue,” journalist Benjamin Ryan writes in The Free Press. “According to internal video and documentation obtained by The Free Press, the organization’s own top brass can’t even align on its official public stance.” In The American Spectator, detransitioner Prisha Mosley was unimpressed: “If the nation’s largest medical association cannot clearly say that minors should not undergo irreversible, dangerous, medically unnecessary surgeries, what exactly does it stand for?”
The proponents of the Affirmative Gender Care are committed to continue their sacred mission regardless of the realities:
. . . It is well established that 80% - 90% of children who satisfy the gender dysphoria diagnostic criteria of will desist by adolescence if nothing is done.
. . . The findings of the referenced Finnish study (along with a multitude of others studies) finds that: Adolescents suffering from GD present with excessive psychiatric morbidity. Subsequent to gender reassignment, psychiatric treatment needs appear to increase. It should be noted that in some individuals, medical GR appears to be linked to deterioration in mental health.