
'Forced to affirm'
Senior psychiatrists in Australia call for a national inquiry into youth gender clinics


Psychiatrists have been forced by the “gender-affirming” treatment model to choose between exposing transgender-identifying children to harm or putting their job at risk, according to a senior Australian child and adolescent psychiatrist, Dr Jillian Spencer.
“We entered our field to try to assist children to thrive, but the gender clinics have been set up, and psychiatrists are being forced to affirm the social transition of all children and go along with the idea that puberty blockers and cross-sex hormones will lead to benefit,” Dr Spencer said.
She was speaking at a Sydney forum on Thursday featuring women under pressure for defending sex-based rights, the interests of women and children, and biological reality.
Dr Spencer called for an urgent federal inquiry into the care of youth gender dysphoria, a condition in which children and adolescents report a distressing sense of disconnect between an inner “gender identity” and their birth sex.
She emphasised that she came to this clinical debate with no political or religious affiliation, saying: “I assure you that this is not part of a culture war, this is a really serious child protection issue.”
Video: Dr Jillian Spencer addresses the “Why can’t women talk about sex?” event staged at N.S.W Parliament House, Sydney
‘Follow Cass’
Another prominent child and adolescent psychiatrist, Dr Carey Breakey, who in 1983 founded the first in-patient mental health unit for adolescents in the state of Queensland, has also come out in favour of a national inquiry into the affirmative treatment approach that rules gender clinics in Australia’s public children’s hospitals.
He suggested as a model England’s youth gender dysphoria review led by paediatrician Dr Hilary Cass. Her interim report has highlighted risks with the gender-affirming treatment approach and led to a decision to close the London-based Tavistock clinic, the world’s largest youth gender service.
“But I think that we’ve also got to look at prescribing rates [in Australia], because prescribing of these medications is off-label and not on the PBS [a federal scheme that subsidises and tracks approved medicines],” Dr Breakey told GCN.
Puberty blockers and cross-sex hormones do not have regulatory approval for use with gender dysphoric minors.
Dr Breakey, who is semi-retired, said data from children’s hospital gender clinics alone would not show the true extent of medicalisation, because their long waiting lists would be leading an unknown number of minors to be taken to private doctors for these off-label prescriptions.
There has been an international explosion in the number of teenagers, mostly girls, rejecting their biology and seeking medical interventions to make their bodies resemble the opposite sex.
Under the American-driven affirmation approach, very young children are regarded as experts in their “gender identity”, even if this is in conflict with their sexed body. There is no objective test to diagnose gender dysphoria.
The gender-affirming approach encourages child-led social transition before puberty with new names, pronouns and clothes, an intervention that may lock-in gender distress otherwise likely to ease as the child matures.
In rapidly expanding gender clinics around the developed world, puberty blockers are offered to children as young as age 10-12 to fend off natural but unwanted development, followed by cross-sex hormones meant to be taken for the rest of their lives.
In Australia, girls as young as 15 have undergone double mastectomy, according to Family Court records. The long-term effects of the gender-affirming medical regimen are unknown. Multiple systematic reviews have found the evidence base to be very weak and uncertain. Detransitioners who regret treatment have begun to emerge.
“I think a lot of doctors think [gender-affirming medicine] is crazy, but they are too afraid to speak up. Mayo Clinic just [sanctioned] a doctor who said, hey, testosterone and transgender female athletes, that’s not fair. And he was a famous exercise physiologist, that basically sends a message. You’ve got to be in line with the party establishment thinking on this”—Fox News medical contributor Dr Marty Makary, 17 June 2023
Forced to affirm
At yesterday’s Sydney forum, Dr Spencer said: “We entered our field [as psychiatrists] to try to assist children to thrive, but the gender clinics have been set up, and psychiatrists are being forced to affirm the social transition of all children and go along with the idea that puberty blockers and cross sex hormones will lead to benefit.
“We are not being allowed any professional discretion as to whether that is the right approach.
“It is incredibly distressing to be forced into harming other people’s children, or otherwise face potential loss of one’s career, livelihood or to be cast out of the workplace, as has happened to me.”
In mid-April Dr Spencer was stood down from her job as a senior staff specialist at a public children’s hospital in the Australian state of Queensland, reportedly accused of “transphobia” after an interaction with a young patient from the gender clinic.
She cannot speak publicly about her employment, but colleagues told The Australian of their concern at the hospital’s handling of her case and its requirement that staff immediately use patients’ opposite-sex pronouns, thereby enabling social transition which some clinicians believe is likely to put young people on a path to lifelong medicalisation.
“I would say that the vast majority of child and adolescent psychiatrists hold very serious concerns about the affirmation model,” Dr Spencer said at the Sydney forum.
“But to speak up in the current climate, or even to take a more cautious clinical approach puts their employment at risk.
“Their [professional] registration is at risk and they fear criminal sanctions under the ‘conversion therapy’ laws in some states.
“I think it is only a very small group of doctors who believe in the affirmation model, but they’re supported by a very vocal social movement.”
She said mental health professionals faced “a lot of organisational and social pressure to affirm children.”
“But when we stop to look at the evidence base behind the affirmation model, we find that the studies have major flaws, and they don’t show sufficient benefit to outweigh the risks and the harms.
“The medications used—puberty blockers and cross-sex hormones—are being prescribed by doctors off-label, so that no drug company has had to prove to the regulators that these treatments provide benefits that outweigh the risks and the harm.
“Gender medicine has taken child and adolescent psychiatry by surprise and has put us on the back foot.
“Previously, our discipline always took a developmental approach, which means that the years of childhood and adolescence were understood to be a period of incredible growth and change.
“We didn’t label children with long-term conditions, such as personality disorders, because we knew that a lot of conditions would ease with maturity.
“And indeed, the 11 studies that were conducted before the affirmation model was in use, when they used a ‘watchful-waiting’ approach, found that 60-90 per of children with gender dysphoria became comfortable in their own bodies with maturity.”
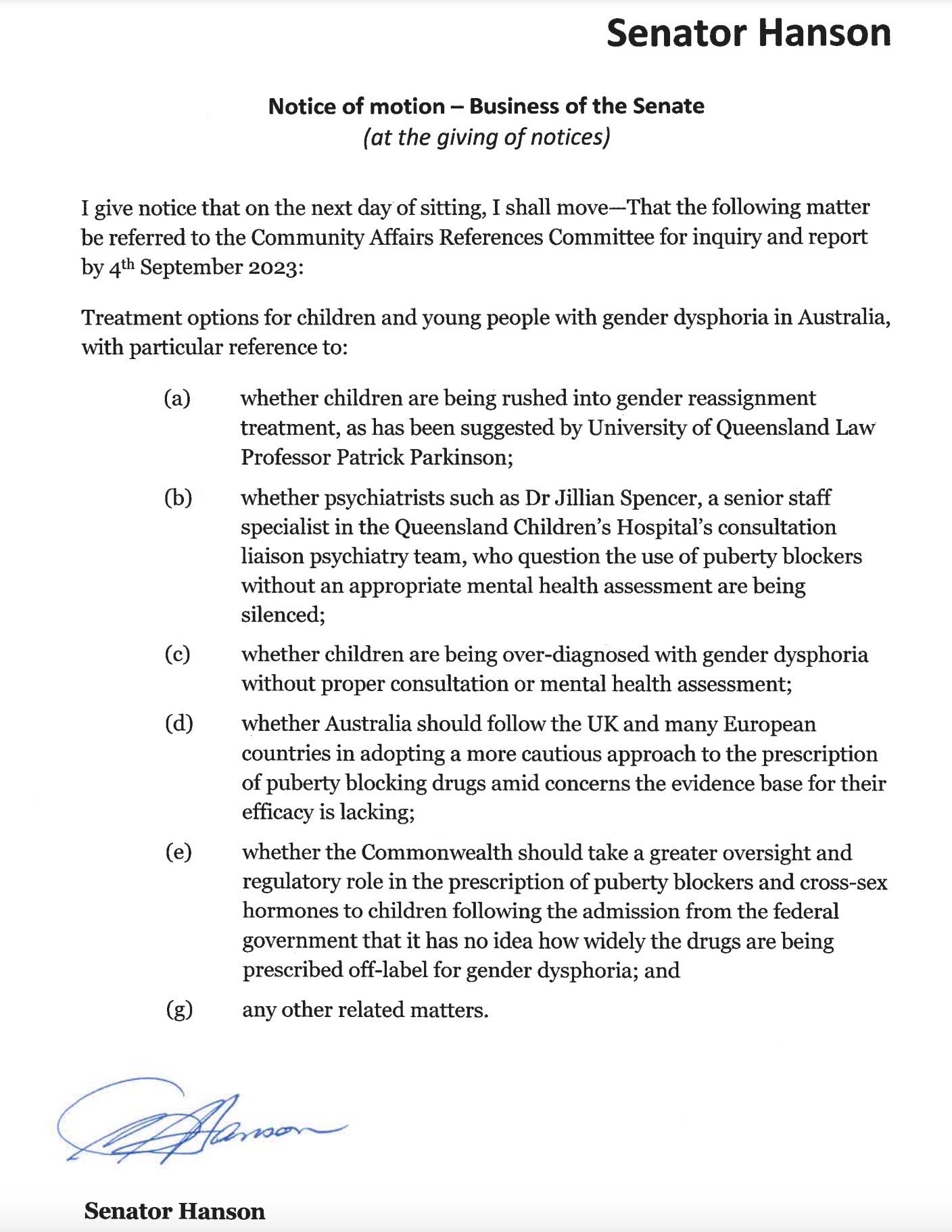
Politics: Pauline Hanson, of Australia’s small One Nation party, has moved a motion for a federal parliamentary committee inquiry into gender clinics. The vote on her motion is expected in the next Senate sittings starting on July 31
Beyond gender
Dr Breakey said that in his 40 years as a child and adolescent psychiatrist, what presented as gender distress often involved underlying problems, including past abuse, which made “growing up as their particular sex risky or undesirable.”
“And if you deal with those [underlying] issues—which can be in the child themselves, or in the family structure, or the culture—then the gender problems go away.”
Dr Breakey believes uncritical gender affirmation prevents this necessary investigation of the child as a whole.
He saw a parallel between anorexia and gender dysphoria, both involving developmental challenges and featuring “waves of presentations”, with this peer network effect amplified by social media.
“Many of the cases of anorexia that we see are kids who are not handling growing up, and the issues of maturing. And I think they’re some of the same issues that are driving the gender dysphoria.”
Dr Breakey also expressed disquiet at what appeared to be health professionals using alarming suicide risk statistics “as leverage to try and get parents to comply [with medical treatment].”
“Child and adolescent psychiatrists work with severely at-risk suicidal kids every day of their week,” he said.
“And dealing with the suicidality is really important, but we do it in the perspective of the whole kid, not just the relationship with gender issues.
“We should deal with the presentation of suicidality in the same way as we would deal with a non gender-disturbed kid with suicidal ideation.”
He agreed with the clinical view that young people in gender clinics would have a level of suicide risk similar to those seeing child and adolescent mental health services for depression, anxiety or autism.
“We shouldn’t be surprised at that, given the number of kids that we see in the gender clinic figures who already have depression, autism, anxiety and so on.”
Dr Jillian Spencer’s professional insight, logic, integrity and willingness to speak the truth has come at great cost. She is deserving of much credit.
Her statement combined with Senator Pauline Hanson’s initiative in parliament will hopefully result in open and honest exposure of just how wrong this stuff really is.
"Puberty blockers and cross-sex hormones do not have regulatory approval for use with gender dysphoric minors."
Or adults! At least in the US.