
Crime scene
Rules broken at Italy's gender clinic; despair over Germany's politicised treatment guideline; a call for caution in Sweden; and the UK's psychotherapy council disentangles itself from bad policy


GCN in brief
An audit of the gender clinic of Italy’s Careggi hospital in Florence has found breaches of rules on the administration of puberty blocker drugs to minors, according to the newspaper La Repubblica. A criminal investigation has been opened and work has started on a new guideline for gender dysphoria treatment.
The Italian Medicines Agency (AIFA) requires dysphoric patients to be given psychiatric support before hormone suppression begins, including specialist child neuropsychiatry. It appears this was not properly done. The Careggi gender clinic also reportedly failed to send mandatory data to AIFA so it could monitor treatment with triptorelin.
AIFA has been asked for a report on the therapeutic indications for this drug, the mainstream uses of which include treatment of hormone-dependent cancer, endometriosis and precocious (premature) puberty.
The full report of the January 23-24 audit of the Careggi clinic by health ministry inspectors has not been released, but some of its findings were detailed in written answers from Italy’s Health Minister Orazio Schillaci to the Senate leader of the Forza Italia party, Maurizio Gasparri, who last December had raised questions about rushed medical treatment.
Earlier this month, Senator Gasparri said: “On the Careggi scandal, I was right. The Tuscan region and the hospital in Florence did not respect the rules set up to protect children. Now those who have harmed minors will have to answer for it.”
He said the health ministry had given the Careggi clinic a list of actions necessary to establish safe treatment, according to the news agency Adnkronos.
“At Careggi, there is no adequate child neuropsychiatry assistance, which is indispensable for managing such delicate events as that of a sex change preceded by the blocking of puberty through medication,” Senator Gasparri said. “This is only the beginning, because this scandal will also have consequences of a criminal nature that are the responsibility of the Public Prosecutor’s Office.”
A copy of the inspectors’ report was sent to the prosecutor’s office in Florence, which has begun a criminal investigation following a complaint by family law expert Annamaria Bernardini de Pace.
About 20-30 minors reportedly begin medicalised gender change each year at the Careggi clinic, and January’s audit involved patient files from 85 cases.
Last month, a roundtable of Italy’s health and family ministries was set up to develop new guidelines for gender dysphoria treatment, starting with puberty blockers, according to the news agency AGI.
This work is to draw on a survey of the scientific literature and the experience of other countries. The National Bioethics Committee has been asked whether the use of triptorelin for gender dysphoria treatment should be reconsidered.
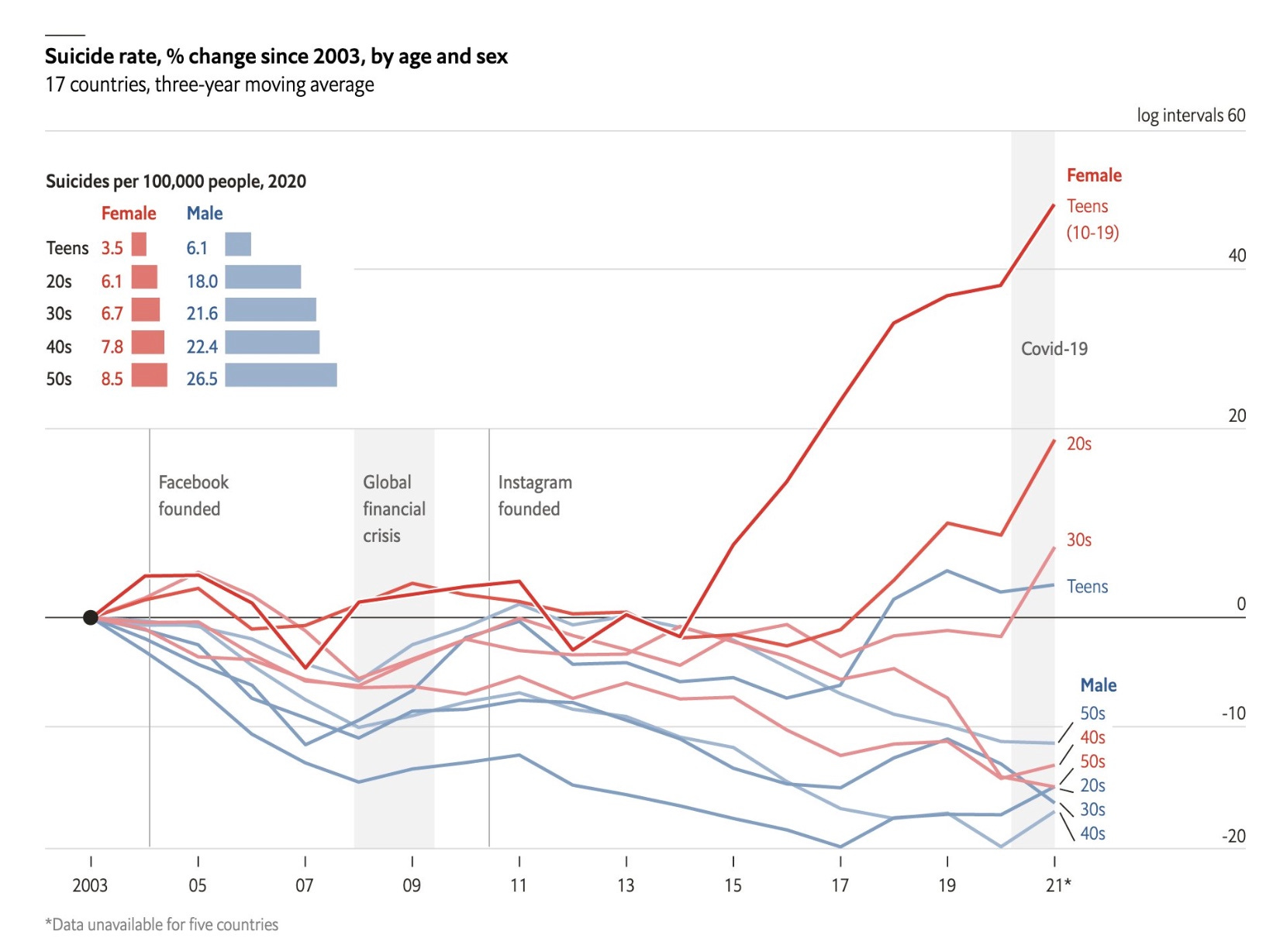
Chart: Note the trend for female teens following the advent of social media platforms
Video: Social psychologist Jonathan Haidt on smartphones, anxious teenagers and group influence in clusters of girls with gender dysphoria. Interview transcript here
Political medicine
Germany’s new “trans-affirmative” guideline is a politicised document that ignores the lack of evidence, according to child and adolescent psychiatrist Alexander Korte, an expert on youth gender dysphoria.
In an interview last month with the German feminist magazine Emma, Dr Korte said the new guideline dispensed with previous advice that cross-sex hormones should generally not be given before age 16 and gender reassignment surgery not before 18.
“These age limits have now been completely removed. In other words, there are no more boundaries for anything! Neither for puberty blockade, nor for opposite-sex hormones, nor for mastectomies or genital surgery,” Dr Korte said.
Dr Korte, a dissenting member of the guideline development group, said earlier treatment advice dating back to 2013 had acknowledged ongoing controversy about puberty blockers, and he pointed out that “the pendulum” had since swung away from routine use of these drugs in countries such as Sweden, Finland and England.
“Nevertheless, Germany continues to treat gender dysphoric children with puberty blockers and, what’s more, these new guidelines are the first treatment recommendations to make this approach a normal treatment option,” he said.
“And anyone who criticises this is put in the right-wing corner. The guidelines untruthfully state that a ban on puberty blockers in Germany is only being demanded by the [populist-right political party] AfD. Even if I share the AfD’s rejection [of puberty blockers], this kind of politicisation does not belong in a medical guideline.”
Dr Korte noted the unusual inclusion of a preamble in the new treatment guideline.
“This is normally only found at the beginning of a constitution or a treaty under international law,” he said. “[It shows] the whole thing is highly politicised and ideologically charged. What was originally a medical problem has become a political issue.
“Significantly, for example, we no longer talk about ‘patients’, but about ‘treatment seekers’. The aim is to depathologise. But treatment seekers is not a term from our social law, because only patients—people with clinically relevant suffering and a disorder worthy of [description as an] illness—have the right to have the costs of their treatment covered by the health insurance funds… This vocabulary, which comes from transgender ideology, is very revealing.”
Dr Korte said the new guideline took the view that mental illness or eating disorders in adolescents could not be triggers for their desire to undergo medicalised gender change, but instead reflected anti-trans discrimination by society.
“This demonstrates a complete lack of understanding of developmental processes in adolescence, especially in pubescent girls. Of course, gender dysphoria is often also a symptom. For example, we observe much more frequently than before that girls whose actual problem is an eating disorder or a feeling of being overwhelmed as a result of the physical changes of puberty are now increasingly convinced that they are ‘trans’.
“Colleagues in specialised eating disorder clinics can tell you a thing or two about this. They report that the majority of patients are now coming round the corner with the trans issue.
“And it is well known that discomfort with one’s own sex and the rejection of one’s own body can also be the result of sexual trauma—so, gender dysphoria is a symptom here too!”
Slow down
A Swedish paediatric endocrinologist has spoken out against a proposal in her country to lower the age for legal gender reassignment to 16 years, without requiring any formal diagnosis. In an opinion article for the newspaper the Gothenburg Post, Jovanna Dahlgren of Gothenburg University argues that the poor outcomes and regret associated with gender reassignment are not well known.
“Those in favour of the new bill certainly believe they are protecting the rights of LGBT people,” Dr Dahlgren said.
“[But] an infrastructure is being built to make it easier for minors to speed up the process of gender reassignment. On the contrary, politicians should invest in more child psychiatric care that examines underlying dysphoria, investigates any concomitant neuropsychiatric disability that may affect the outcome, and strengthens the child’s identity, rather than affirming their thoughts of being ‘born in the wrong body’.
“The scientific situation is complex and evolving. It concerns paediatrics, psychiatry and endocrinology, as well as the evaluation of statistics and scientific evidence.”
She said the Sahlgrenska Academy at her university would hold a symposium on the science of gender dysphoria at the end of August this year. “It will be open to the public. The Prime Minister [Ulf Kristersson] and other members of parliament are welcome to attend and listen to the scientific arguments.”
Include us out
The UK Council for Psychotherapy (UKCP) has withdrawn from the Memorandum of Understanding on Conversion Therapy in the UK (MoU), a document signed by more than 20 health, counselling and psychotherapy associations.
Critics of the MoU see it as a vehicle for influence by trans activism and the dogmatic “gender-affirming” treatment approach. Internationally, there is concern that ill-designed restrictions on “conversion therapy” deemed to target “gender identity” may deny adolescents perfectly ethical psychological interventions during a period of profound change and development.
In a statement, UKCP attributed its decision to withdraw from the MoU to confirmation that the document did indeed apply to minors, contrary to previous assurances. “Without the involvement of and full consultation with UKCP child psychotherapists and child psychotherapeutic counsellors, UKCP would not have signed the MoU if it was known to relate to children,” UKCP said.
“Due to the complexities relating to working with children and young people, UKCP believes that separate guidance is needed for such clients/patients and must be very carefully thought through.”
UKCP advised its members to no longer regard the MoU as its policy.
The group Critical Therapy Antidote, which opposes politicisation of healthcare, said the shift was very significant, UKCP being the first professional body to push back against the ideological capture of the MoU.
“Control of the MoU is in the hands of a small group of activist therapists called the Coalition Against Conversion Therapy, chaired by [non-binary psychologist] Dr Igi Moon,” the group said.
“The MoU is committed to gender identity ideology which rejects the biological base of sex. There are key similarities to [the World Professional Association for Transgender Health] in that both are hybrid organisations which frame exploratory therapy as problematic and are committed to pursuing comprehensive re-education of health professionals on ‘intersectionality’.”
Apologies in advance for a comment that is somewhat off topic, in relation to the subject matter of this GCN article, hopefully it has some relevance:
Examples of the endlessly regurgitated shock-horror’ announcements in our news outlets:
• “New Study Reveals Shocking Rates of Attempted Suicide Among Trans Adolescents”
• “Why have nearly half of transgender Australians attempted suicide?”
• “More than 40% of transgender adults in the US have attempted suicide.”
• “The suicide attempt rate among transgender persons ranges from 32% to 50% globally.”
• “Data indicate that 82% of transgender individuals have considered killing themselves.”
Despite their newsworthiness I can find no evidence of a single child or adolescent trans suicide in Australia. By way of contrast there is a wealth of information available confirming that indigenous adolescents have a suicide rate that is four times that of their non-indigenous counterparts (ref: Australian Institute of Health & Welfare).
A British study calculated the annual suicide rate for Trans children between 2010 – 2020 as 13 per 100,000 (Office of National Statistics 2021). A paper by Dixon et al in the NT. J. Environ. Res. Public Health 2019 calculated the (non-trans) Indigenous adolescent suicide rate as 35.6 to 57.50 per 100,000.
. . . . . Yet no headlines of indigenous suicide, no outrage and not fraction of the concern or resources that are dedicated to the “Shocking Rates of attempted Suicide” in the Trans community.