Heavily promoted long-term studies involving youth gender clinics are unlikely to produce the rigorous data needed to prove the outcomes and safety of the “gender-affirming” treatment approach, according to an analysis in the prestigious journal Archives of Sexual Behavior.
The analysis by psychiatrist Dr Alison Clayton argues that the weak “observational” design of current high-profile studies in the United States and Australia means they will be prone to bias and unable to distinguish treatment outcomes from placebo influences, such as the positive effect on patient wellbeing that comes with attention from motivated clinicians.
“The aims of these studies are to provide the urgently needed rigorous empirical data to bolster the weak evidence base that currently underpins the [gender-affirming treatment] approach [but these studies are] unlikely to provide the rigorous empirical data that can convincingly demonstrate a causal relationship between treatment and outcome,” she says.
The purpose of the Clayton analysis is to stimulate urgent debate among experts in research methodology on how to design more robust, ethical studies capable of resolving serious uncertainties in youth gender dysphoria care. The analysis may also be relevant to future litigation, and to planning and research by England’s Cass review.
The gender-affirming treatment approach takes its lead from the self-declared “gender identity” of children and adolescents, and promotes both early social transition for children to live as the opposite sex, as well as medical interventions ranging from puberty blockers through opposite-sex hormones to transgender surgery, such as mastectomy.
Placebo effects in this field would be positive psychological outcomes caused by the clinical or research context, not by the treatment itself.
Dr Clayton documents the risks of gender-affirming interventions, including possible interference with a critical window for brain development and permanent infertility as adults.
“Children as young as ten, who do not have capacity for informed consent, are starting a treatment course that will likely render them infertile or sterile and this raises complex bioethical issues,” she says.
Video: Neuroscience and the placebo effect
No better than a sugar pill
Puberty blockers and opposite-sex hormone drugs promoted as “lifesaving” by gender clinics may be no better than inert placebo pills.
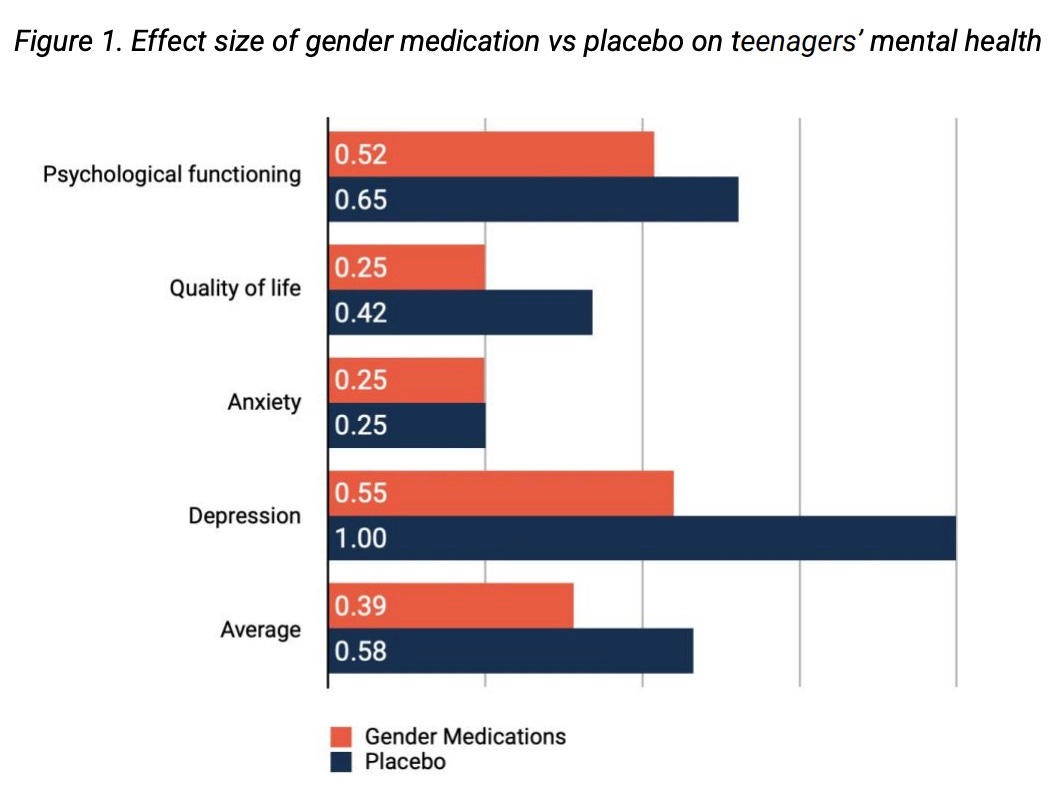
A new technical paper published today by the London-based organisation Sex Matters concludes that these gender medications are less beneficial than placebo for a young patient’s psychological functioning, quality of life and depression.
“This study shows that the gender-affirmative medical model for teenagers is based on faulty assumptions, and may do more harm than good,” says the paper’s author, Matilda Gosling, an independent social research consultant.
Unlike a placebo pill, the hormonal interventions of gender clinics come with risks including low bone density, cardiovascular problems, and loss of sexual function. The interventions rest on a weak and uncertain evidence base.
“Evidence showing positive mental health impacts [after gender medications] ought reasonably to be greater than placebo at worst, and overwhelming at best, to justify these physical impacts,” the paper says.
Given the lack of any experimental studies directly calculating the placebo effect for gender medications, Ms Gosling used the demonstrated placebo effect of other medications for mental health conditions such as depression.
She compared the size of this placebo effect with the average improvements in mental health reported by longitudinal studies of young patients given puberty blockers and hormone drugs.
The mental health profile of adolescents with gender dysphoria is similar to peers referred to mental health services for other conditions.
“Analysis of current research demonstrates that gender medications, in the form of puberty blockers and hormone treatment, are not any better than taking a placebo in positively affecting teenagers’ mental health,” the paper says.
“The limited available data suggests they may be worse. Follow-up research in this area is urgently needed, including a full meta-analysis.”
Gender medication means puberty blockers and/or opposite-sex hormone drugs. The comparison was made using studies since 2010. Source: Sex Matters
The Sex Matters paper was written in the knowledge that its results would come under “an unusual degree of scrutiny”, so full tables and literature search terms are included to enable re-analysis by others.
The paper also discloses limitations including reliance on many studies of patients with early-onset gender dysphoria. Today’s gender clinics are dominated by adolescent-onset cases, for whom there is very little outcome data.
Another limitation was the poor quality of gender medication research claiming beneficial outcomes — “There are small sample sizes, high levels of attrition, meaningless comparison groups and a degree of obfuscation in reporting of results,” the paper says.
Gender Clinic News is a reader-supported publication. To receive new posts and support my work, consider becoming a free or paid subscriber.
Promising data ahead?
Some gender clinicians in the U.S. who concede the lack of good-quality evidence for their interventions have talked up the prospects of a multi-clinic study led by Dr Johanna Olson-Kennedy, who runs the gender clinic at the Children’s Hospital Los Angeles.
The 2019 research protocol says this study will collect “critical data on the existing models of [gender-affirming] care for transgender youth that have been used in clinical settings for close to a decade, although with limited empirical research to support them.”
In Australia, the Trans20 research project is being conducted at the Royal Children’s Hospital Melbourne (RCH), where the gender clinic director is Dr Michelle Telfer. In their 2019 study protocol, the Trans20 researchers declare “an urgent need for more evidence to ensure optimal medical and psychosocial interventions” with minors.
The researchers say that “ethical reasons” prevented the use of an untreated control group, and they concede this less than ideal design “will limit the potential to draw direct conclusions about the effectiveness of interventions.”
They say that “where possible” they will use measures with population-based data to compare treatment outcomes of Trans20 patients with those of the general population.
It is not clear whether the researchers considered the use of a comparison group of patients given an alternative to gender-affirming treatment, such as exploratory psychotherapy or trauma-informed therapy.
In her analysis published last month in the Archives of Sexual Behavior — edited by clinical psychologist Dr Kenneth Zucker, a leading international authority on youth gender dysphoria — Dr Clayton argues that gender clinics have created “a perfect storm setting” for placebo effects with unbalanced “celebration” of the gender-affirming approach in both clinical and research environments.
“We have a population of vulnerable youth presenting with a condition [gender dysphoria], which has no objective diagnostic tests, and that is currently undergoing an unexplained rapid increase in prevalence and marked change in patient demographics,” she says.
“The treatment response is mainly based on patient-reported outcomes.
“Some clinicians, who may be affiliated with prestigious institutions, enthusiastically promote [gender-affirming treatment], including on the media, social media, and alongside celebrity patients.
“Some make overstated claims about the strength of evidence and the certainty of benefits of [gender-affirming treatment], including an emphasis on their ‘life-saving’ qualities, and under-acknowledge the risks.
“Alternative [non-medical] psychosocial treatment approaches are sometimes denigrated as harmful and unethical conversion practices or as ‘doing nothing.’
“This combination of features increases the likelihood that there will be a complex interplay of heightened placebo and [harmful] nocebo effects in this area of medicine, with significant implications for research and clinical practice.”
Failed replication
In the field of youth gender dysphoria, there have been no randomised controlled trials — the gold standard for proving the causal link between treatment and outcome — nor comparison studies pitting gender-affirming medical interventions against less risky alternatives for minors, such as the “watchful waiting” approach.
In 2019, it emerged that researchers planning a 2011-14 puberty blocker study at England’s Tavistock gender clinic had initially been refused ethics clearance because they were not open to using a randomised control design that would allow firm conclusions about the effect of this early suppression of puberty.
The researchers — who hoped to achieve the first replication of the positive results of a pioneering Dutch study which inspired international adoption of puberty blockers — objected that patients assigned to a Tavistock no-treatment control group would buy blockers online.
A second ethics committee then approved the Tavistock study’s weaker, observational design. After the release of some discouraging preliminary data, the full results were not published until 2020, following a sustained campaign for transparency.
The key finding at the Tavistock was one of no change in psychological function or gender dysphoria after puberty blockers. Had a change been reported, it could not have been attributed to the blocker intervention with confidence, given the lack of a control group or a group given alternative treatment.
In her analysis Dr Clayton says that gender-affirming interventions have been introduced as routine clinical treatments, despite their weak evidence base, with “catch-up research” now supposed to remedy the lack of good quality data.
But she says this research gives rise to difficult dilemmas if undertaken in “a placebo-effect-enhancing clinical environment”, rather than a robust research environment controlling for placebo influences.
“There seems to be a problematic tension between the research and clinical agendas of [youth gender clinics],” she says.
“[Gender-affirming treatment] is being provided in a clinical environment that maximises the placebo effect.
“This is the same environment in which the same clinicians are researching [the efficacy of gender-affirming treatment].
“A medical profession that does little to distinguish placebo effects from specific treatment effects risks becoming little different from pseudoscience and the quackery that dominated medicine of past times, with likely resulting decline in public trust and deterioration in patient outcomes.”
Dr Clayton, a Melbourne researcher affiliated with the Society for Evidence-based Gender Medicine, cites the Australian Trans20 study at the RCH Melbourne gender-affirming clinic as an example of the difficulties posed by placebo-enhancing contexts.
“It is important to highlight that this study’s human research ethics committee (HREC) approval was not for the treatment approach, which was implemented as routine clinical care, rather it was for matters such as collection and storage of data, and longitudinal follow-up of discharged patients,” she says.
She says RCH secured HREC approval in 2019 for a “newsletter blog” to be sent to gender clinic patients and families in order to boost patient engagement with the Trans20 study; this was said to raise no new ethical issues.
But Dr Clayton points out that this request for help with the clinic’s flagship research project came with upbeat accounts of the clinic, its services and patients on the gender transition path.
“For example, following attendance at the clinic’s single-session assessment triage (SSNac) young people were described as feeling ‘empowered ... and more likely to start living as their preferred gender,’ and having improvements in mental health and quality of life,” she says.
“A colourful diagram showed the increased rates of social transition that followed SSNac attendance, and the section concluded ‘Hopefully the improvements after SSNac are a taste of things to come!’ ”
“There was a ‘lived experience’ piece in which a well-known transitioned, now young adult, patient was pictured receiving an award. This patient provided a personal testimony of the clinic’s medical director: She ‘will always be one of my biggest heroes...an incredible person: Intelligent, compassionate and strong’.”
Dr Clayton says that “sandwiching the requests for a research survey completion between celebratory accounts of the clinic seems likely to magnify the impact of bias and placebo effect on research outcome findings.”
She says the consequences may include —
bias if patients want to please a clinician by giving positive reports of treatment outcomes
bias because patients with positive experiences of the clinic are more likely to complete research surveys
social learning and emotional contagion when symptoms spread among patients in clinical trials
expectations of patients being influenced by the social prestige of clinicians
positive outcomes as a result of the special attention received by patients (but wrongly attributed to treatment)
Apart from the RCH newsletter’s effect on research, Dr Clayton wonders whether it represents “ideal clinical practice.”
“Think, for example, of the young [gender dysphoria] patient who may be hesitant to transition. Where is the celebration of this young person’s choices?,” she says.
“Communications from the clinic, such as this newsletter, may contribute to feelings that, unless he/she transitions, he/she lacks courage (having not been ‘empowered’) and that he/she will never be an award-winning celebrated patient.
“This may act as a covert form of pressure on patients to transition or, for those who do not, act as a nocebo effect negatively impacting their psychological outcomes.”
Note:GCN sought comment from RCH and Dr Telfer. In 2019, the hospital said its gender clinic treatment was based on the “best available medical evidence”, in line with “international best practice”, and followed “strict clinical governance standards”. GCN does not dispute that gender-affirming clinicians believe their interventions are of benefit to vulnerable patients in distress.
Ever more healthy young people diagnosed with gender dysphoria (GD) are lining up for un-trialled, irreversible surgical and hormonal therapy in order to ‘change their gender’.
There is a distinct possibility that the current protocols for managing GD could turn out to be a dreadful mistake.
For this reason, to give some context to the ‘mistake’ concept, I list a few (of the many) historical examples:
Frontal Lobotomy:
Portuguese neurologist Egas Moniz performed the first such procedure to treat refractory psychiatric conditions in 1935. The last recorded lobotomy in the Western world was in the U.S. in 1967. Lobotomy left many patients worse off following surgery, many died and many who survived were left in a vegetative state.
Number of damaged patients: Probably in excess of 100,000.
Time to abolition: 31 years
Thalidomide:
First marketed in West Germany in 1956 as an over the counter medication to treat anxiety, insomnia and hyperemesis gravidarum (‘morning sickness’). Concerns regarding birth defects in infants born of mothers taking the drug soon became apparent; this included stillbirth, grotesque limb malformations and major organ system damage.
Number of damaged patients: 10,000 – 20,000.
Time to abolition: 5 years
Pelvic mesh implant:
A very recent disaster: This device was approved by the FDA in 2002 for repair of pelvic organ prolapse, a not uncommon problem following pregnancy. Some 150,000 women in Australia were treated thus. Delayed outcomes revealed a litany of disastrous irreversible effects including erosion into the bladder and vagina, dyspareunia, urinary fistula and systemic immune conditions.
The device was withdrawn by the Australian TGA in November 2017.
An Australian class-action suit (the largest of its kind) began in 2017 while the current global total settlements approaches US$8 billion.
Number of damaged patients: 150,000 -200,000
Time to abolition: 15 years
The above three examples had not undergone any form of clinical trial to establish efficacy and safety.







That does seem short for follow-up. And as far as I know, they are not testing gender-affirming treatments against any alternative treatment approach.
Ever more healthy young people diagnosed with gender dysphoria (GD) are lining up for un-trialled, irreversible surgical and hormonal therapy in order to ‘change their gender’.
There is a distinct possibility that the current protocols for managing GD could turn out to be a dreadful mistake.
For this reason, to give some context to the ‘mistake’ concept, I list a few (of the many) historical examples:
Frontal Lobotomy:
Portuguese neurologist Egas Moniz performed the first such procedure to treat refractory psychiatric conditions in 1935. The last recorded lobotomy in the Western world was in the U.S. in 1967. Lobotomy left many patients worse off following surgery, many died and many who survived were left in a vegetative state.
Number of damaged patients: Probably in excess of 100,000.
Time to abolition: 31 years
Thalidomide:
First marketed in West Germany in 1956 as an over the counter medication to treat anxiety, insomnia and hyperemesis gravidarum (‘morning sickness’). Concerns regarding birth defects in infants born of mothers taking the drug soon became apparent; this included stillbirth, grotesque limb malformations and major organ system damage.
Number of damaged patients: 10,000 – 20,000.
Time to abolition: 5 years
Pelvic mesh implant:
A very recent disaster: This device was approved by the FDA in 2002 for repair of pelvic organ prolapse, a not uncommon problem following pregnancy. Some 150,000 women in Australia were treated thus. Delayed outcomes revealed a litany of disastrous irreversible effects including erosion into the bladder and vagina, dyspareunia, urinary fistula and systemic immune conditions.
The device was withdrawn by the Australian TGA in November 2017.
An Australian class-action suit (the largest of its kind) began in 2017 while the current global total settlements approaches US$8 billion.
Number of damaged patients: 150,000 -200,000
Time to abolition: 15 years
The above three examples had not undergone any form of clinical trial to establish efficacy and safety.