
Blocked & retorted
Clinicians debunk the Endocrine Society's suicide prevention claim with its own words


The gist
There is no good evidence that medicalised gender change prevents suicide, and politicised medical societies are exaggerating the benefits of these medical interventions while playing down the risks.
This is the claim in a damning letter today in The Wall Street Journal from 21 clinicians and researchers from nine countries involved in direct care of the fast-growing numbers of teenagers presenting with gender distress.
The signatories, including the prominent psychiatrists Prof. Riitakerttu Kaltiala of Finland and Prof. Stephen B. Levine of the United States, were responding to a July 5 letter to the editor from the Endocrine Society’s president Dr. Stephen R. Hammes.
Puberty blockers, which suppress natural sex hormones, and cross-sex hormones given to masculinise or feminise the body, fall within the expertise of endocrinologists.
In defence of the society’s 2017 treatment guideline, which is invoked internationally to justify hormonal interventions for minors who identify as transgender or non-binary, Dr. Hammes had claimed that more than 2,000 studies showed such “gender-affirming” treatment improved well-being and reduced suicide risk.
But the July 14 letter from Prof. Kaltiala and her colleagues turns the tables on the society, saying—
“Dr. Hammes’s claim that gender transition reduces suicides is contradicted by every systematic review [of the evidence base], including the review published by the Endocrine Society, which states, ‘We could not draw any conclusions about death by suicide.’
“There is no reliable evidence to suggest that hormonal transition is an effective suicide-prevention measure.”
Evidence doesn’t add up
The Hammes letter said nothing of the quality of those 2,000-plus studies; quality that can be measured in a reliable and reproducible way by a systematic review of the evidence base for paediatric gender transition.
“Every systematic review of evidence to date, including one published in the Journal of the Endocrine Society, has found the evidence for mental-health benefits of hormonal interventions for minors to be of low or very low certainty,” says the letter from Prof. Kaltiala and colleagues.
“By contrast, the risks are significant and include sterility, lifelong dependence on medication and the anguish of regret.
“For this reason, more and more European countries and international professional organizations now recommend psychotherapy rather than hormones and surgeries as the first line of treatment for gender-dysphoric youth.”
Other signatories from the group of 21 clinicians and researchers include—
Clinical psychologist Dr. Anna Hutchinson and family psychotherapist Dr. Anastassis Spiliadis (both former internal critics of hasty medicalisation at the London-based Tavistock gender clinic)
Swedish child psychiatrists Dr Sven Román and Dr Angela Sämfjord
The director of Belgium’s Centre for Evidence-Based Medicine Dr. Patrick Vankrunkelsven
Psychologist Prof. Celine Masson and child and adolescent psychiatrist Dr. Caroline Eliacheff (co-founders of the French watchdog group the Little Mermaid)
American endocrinologist Dr. William Malone (director of the Society for Evidence-Based Gender Medicine)
Florida paediatrician and bioethicist Prof. Patrick K. Hunter
The detail
Eminence-based medicine
The Hammes letter also cited policies from “reputable” medical societies such as the American Academy of Pediatrics (AAP) in favour of the gender-affirming treatment approach with its hormonal and sometimes surgical interventions for young people.
However, the AAP’s 2018 policy on gender dysphoria has been subjected to a withering and unrebutted “fact check” by clinical psychologist and researcher Dr. James M. Cantor, who says the studies cited by the AAP contradict its affirmation-only position and in fact endorse the more cautious approach of “watchful waiting” that it discourages.
The AAP also stands accused of blocking requests from concerned paediatrician members for open discussion about gender dysphoria care and for a proper systematic review of the evidence, which was not undertaken before adoption of the 2018 policy.
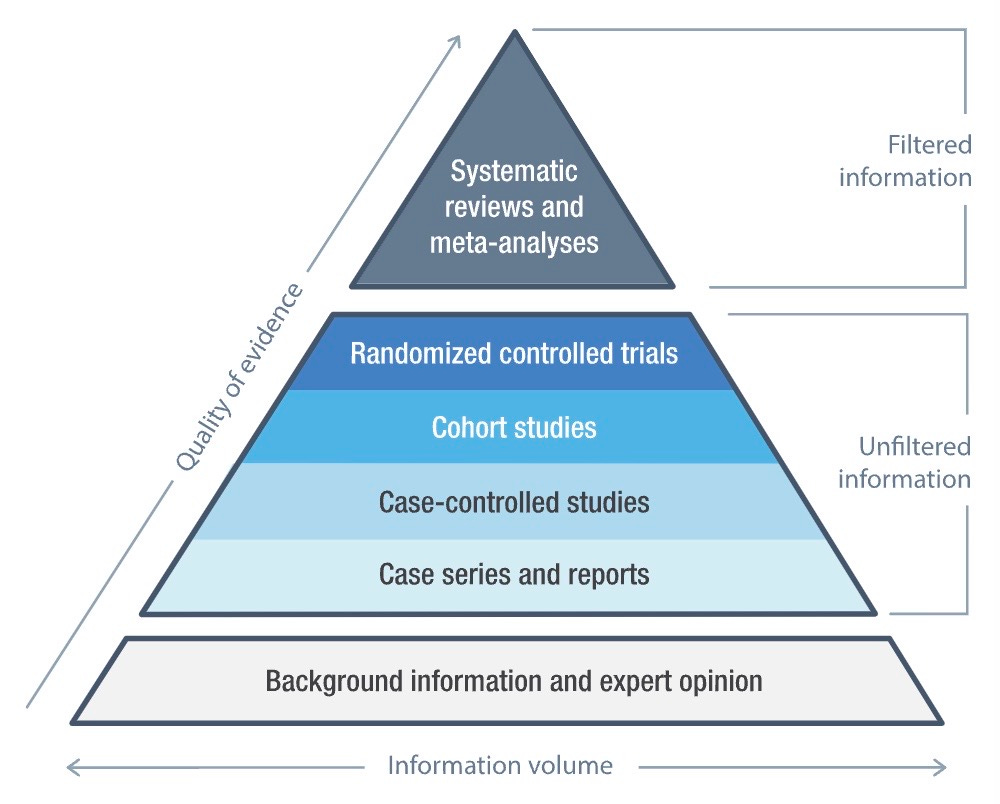
Especially since 2020, when Finland published the first cautious treatment policy based on a systematic review, the gender-affirming lobby has sought to deflect questions about the evidence base by relying on treatment guidelines and statements from medical societies devised by small committees open to ideological capture. These documents represent expert opinion, which occupies the low-quality base of the evidence pyramid, while systematic reviews are placed at the apex.
Finland’s lead has been followed with systematic reviews in Sweden, the United Kingdom and the American state of Florida, all concluding that the evidence base is very weak and uncertain.
Graphic: Not all evidence is equal
False consensus
In his letter, Dr. Hammes had responded to what he termed political “misinformation” in a June 28 opinion article in The Wall Street Journal by endocrinologist Dr. Roy Eappen and data scientist Dr. Ian Kingsbury from Do No Harm, a group opposed to extreme identity politics and gender ideology in healthcare.
Drs. Eappen and Kingsbury, together with Californian detransitioner Chloe Cole, fronted up to the Endocrine Society conference in Chicago last month, and engaged attending endocrinologists in discussion of gender dysphoria care.
“Without exception, they acknowledged that the society’s evidence base for pediatric gender transition is weak, at best,” Drs. Eappen and Kingsbury wrote in their WSJ article headlined “The Endocrine Society’s Dangerous Transgender Politicization.”
“Yet while they’re aware of the guidelines’ shortcomings, they’re afraid to voice their concerns. The society’s full-throated endorsement of gender-affirming care implied condemnation of anyone who holds differing views.
“Medical professionals are being cowed into silence and coerced into providing treatments they know are dangerous to children.”
The authors claimed that the Endocrine Society and other associations of health professionals had been “co-opted” by trans activists, resulting in treatment guidelines “based on flimsy evidence” and misrepresenting irreversible interventions as beneficial for young people.
Video: Destransitioner Chloe Cole got the message that if she didn’t transition she’d be at risk of suicide
American exceptionalism
In their WSJ article, Drs. Eappen and Kingsbury said their “most telling interactions” at the Endocrine Society meeting in Chicago were with endocrinologists from Europe.
“Those we spoke with expressed surprise that the U.S. hasn’t banned, or at least severely restricted, such treatments for adolescents and children,” they wrote.
“England, Sweden and Finland have all taken this path, and Norway is likely to follow. Belgium, France, Ireland and Italy are also raising concerns. These countries are following the science, which shows that the claimed benefits of hormonal intervention for young people fail to outweigh the risks.
“Most disturbing, endocrinologists on all sides of this debate told us that practitioners aren’t complying with the precautions set forth in the society’s guidelines.
“Despite the document’s call for careful mental-health screening and its acknowledgment that most cases of childhood gender dysphoria naturally resolve during puberty, endocrinologists recognize that some of their peers are rushing young patients to irreversible hormonal treatments.
“Every endocrinologist we spoke with supports doing more to ensure that these guardrails are enforced, and many favor erecting new ones.”
Chloe Cole, a young adult detransitioner who was prescribed puberty blockers and testosterone at age 13, said her conversations with practitioners at the Endocrine Society meeting had gone “incredibly well.”
“Nearly everyone who I spoke to about my experience of transitioning as a minor was shocked and disgusted to hear that their own profession is medically transitioning children so flippantly, yet refusing to take care of them after they come to realize the iatrogenic harm the treatments have caused them,” she told GCN.
She said this kind of response challenged the idea that paediatric transition was “a widely accepted practice amongst doctors”.
GCN understands that one influential member of the Endocrine Society’s board has sought to dismiss the European shift to caution as orchestrated by Christian right-wing extremists. The Society for Evidence-Based Medicine has also been smeared as anti-trans and far-right; no proof is offered
Dr. Kingsbury, research director for Do No Harm, said the claim that the gender-affirming model was settled science made it very difficult for U.S.-based medical societies to acknowledge the import of systematic evidence reviews and more cautious treatment policy in Finland, Sweden and England.
“As soon as [those medical societies] reckon with the reality that that consensus doesn’t even extend to three of the world’s most liberal countries, [they have] got a major problem,” he told GCN in an interview.
He said the question was how to get these societies to acknowledge publicly the significance of the cautious turn in Europe.
Do No Harm had its own stand at the Endocrine Society’s Chicago conference—armed with literature including Hannah Barnes’s book “Time to Think: The Inside Story of the Collapse of the Tavistock’s Gender Service for Children”—and practitioners could approach and strike up a conversation.
Dr. Kingsbury’s impression was that amid America’s tribal politics, some advocates of the gender-affirming way at the conference had never before been challenged by secular, politically moderate critics familiar with the evidence base and raising substantive concerns.
He said this was productive and worth repeating.
Video: Florida paediatrician and bioethicist Dr. Patrick Hunter on the low quality of gender-affirming studies published by top peer-reviewed journals
Risk of over-treatment
The Endocrine Society’s 2017 guideline is often cited without revealing its acknowledgement that the hormonal interventions it recommends are largely based on evidence rated as “low” or “very low” quality.
An investigation by the British Medical Journal applied the standards of evidence-based medicine to the treatment guidance offered by the Endocrine Society, the AAP and the World Professional Association for Transgender Health (WPATH). All three documents were found wanting.
In a commentary piece, the journal’s editor-in-chief Dr. Kamran Abbasi noted the divergence in practice between European countries and the U.S., where “more and more young people are being offered medical and surgical intervention for gender transition, sometimes bypassing any psychological support.”
He said that “closer inspection” of the guidance from prominent U.S.-based medical societies “finds that the strength of clinical recommendations is not in line with the strength of the evidence. The risk of over-treatment of gender dysphoria is real.”
Earlier this month, The Australian newspaper’s journalist Natasha Robinson revealed that serious reservations about gender medicine expressed by Australian endocrinologists were not passed on to the then federal health minister, Greg Hunt, who in 2019 had asked the Royal Australasian College of Physicians (RACP) to review gender clinic treatments following media coverage.
In its 2020 public letter of advice to Mr Hunt, the RACP noted it had consulted the Endocrine Society of Australia (ESA) but did not inform the minister of the society’s concerns.
The Medical Affairs Committee of the ESA put its position to the RACP in a 2019 confidential letter, and opposed any endorsement of the 2018 “Australian Standards of Care and Treatment Guidelines” for gender dysphoria issued by the Royal Children’s Hospital Melbourne (RCH), which is home to the country’s most influential gender clinic.
Those treatment guidelines helped to spread and entrench the gender-affirming treatment approach across Australia’s federation.
The ESA committee wrote: “This is a complex area, the evidence base is limited and the RCH document largely reflects the authors’ opinion because, as the authors themselves state, ‘the [scarcity of high-quality] published evidence on the topic prohibited the assessment of level (and quality) of evidence for these recommendations’.”
In its advice to Mr Hunt, however, the RACP praised the RCH guidelines, saying—
“We acknowledge the considerable work, expertise and consultation that took place in the development of these clinical guidelines. The RACP supports the principles underlying these guidelines, specifically the emphasis on a multidisciplinary approach to providing person-centred care which prioritises the best interests, preferences and goals of the patient.”
The RACP did not describe gender clinic treatments nor discuss any possible harm they might do. Instead, the college claimed that the national inquiry urged in the media at the time by some health professionals would “harm vulnerable patients and their families through increased media and public attention.” It provided no evidence for this claim.
It emerged that the RACP had previously lobbied for easier access to the hormonal treatments it was called upon to review.
The RACP’s 2020 advice to the minister was welcomed by RCH chief executive John Stanway and chairman Rob Knowles, who said it had “validated” the work of Dr. Michelle Telfer, the director of the hospital’s gender clinic and lead author of the 2018 treatment guideline.
In its confidential letter to the RACP, obtained by The Australian, the ESA Medical Affairs Committee included comments by an external reviewer, who said—
“The RCH approach claims to set Australian Standards, but the document represents solely the attitudes of one group of advocates in one institution.
“There are gaps in the evidence that the RCH document does not adequately address, one instance being the statement that [hormone suppression drugs used off-label] to block puberty progression are reversible.
“The evidence in children for that statement is limited: one review is cited of long-term follow-up of children treated with [hormone suppression drugs] for central precocious [or premature] puberty. For boys, that summarises the only four very small, disparate and inconclusive studies available, two of which describe no long-term follow-up and none showed any meaningful evidence of ‘full reversibility.’
“RCH advocacy for an affirmative model is, in effect, accepting a child’s wishes as unassailable and implies that any parental reluctance to accept the diagnosis of gender dysphoria and its treatment is ill-informed resistance to be overcome by goal-oriented ‘counselling.’ The RCH argument that non-treatment in the face of gender dysphoria is not neutral, uses an exaggerated risk of suicidality to make this unbalanced argument seem necessary.
“The RCH document does not address the real problem of differentiating genuine gender dysphoria (with early onset of unshakeable belief that the person was born and raised into the wrong sex) from others who are gender-confused children or adolescents who consider themselves ‘non-binary’, ‘gender-fluid’, ‘agender’, ‘third gender’, etc. Such features may connote youthful, yet-to-mature understanding of sex and gender.
“One view is that the latter should not be treated with puberty blockers or cross-sex hormones at least until adulthood and then only on the advice of an experienced psychiatrist and/or psychologist as part of a transgender medicine multidisciplinary team.”
On July 7, the Endocrine Society of Australia tweeted that it “supports gender-affirming care in keeping with the latest evidence as summarised” by WPATH’s standards of care, the Endocrine Society guideline and medical society statements.
Note: GCN has sought comment from the Endocrine Society, the Royal Australasian College of Physicians, the Endocrine Society of Australia and RCH. GCN does not dispute that gender-affirming clinicians genuinely believe their interventions help vulnerable young people
There seems to be something incongruous in the gender dysphoria suicide risk as it relates to the realities of childhood suicides in Australia:
Australia’s ‘Children’s Research Institute’ website estimates that approximately 1.2% of Australian school children (approx. 45,000) identify as trans. I have searched extensively for statistics on the number of Australian childhood suicides associated with gender dysphoria but cannot find a single reference.
The Australian Bureau of Statistics quotes the age-specific death rate for Aboriginal and Torres Strait Islander child suicide is 8.3 deaths per 100,000, translating as approximately 4 per 45,000.
It is interesting to note there is a highly publicised group said to be at great risk of suicide (with either few or no documented cases) undergoing an experimental, irreversible, sterilising and mutilating procedures to address mental health challenges. Meanwhile, it seems there is little public awareness being raised of another group of children with well documented horrific rates of suicide..
If childhood suicide prevention is the primary concern then they’ve picked the wrong cohort!
But still we persist in following the flawed RCH guidelines in Australia.
Multiple reviews have debunked the main evidence base( the Dutch studies)
When is the RACP going to admit its mistake in endorsing the RCH guidelines?
How many more children are going to be harmed in this country before we come to our senses?